Pain Management and Palliative Care in Sub-Saharan Africa: Reflections From Uganda
Pain management is a subspecialty still in development in much of sub-Saharan Africa. Access to providers and medications is severely constrained over much of the region. Cultural factors, such as mistrust both of providers and concerns regarding opioid use, also act as barriers to care. Although some academic anesthesia training programs exist,[1] the majority of palliative and anesthesia care in Uganda is provided by individuals who have limited formal medical or nursing training.[2] Regional anesthesia is largely unknown,[3] and access to pain medications is severely constrained. As a result, pain management training has been limited to the palliative care setting.
“An estimated 57% of Ugandans do not have access to health care and some 250,000 are in need of palliative care to improve their quality of life.”
Palliative care was introduced in Uganda in 1993 by Dr Anne Merriman, founder of Hospice Africa Uganda (HAU) in Kampala. HAU is a nongovernmental organization that provides support and care to those dying from cancer and HIV/AIDS. Over the past few decades, services have expanded to include affiliated clinics in two other districts as well as training programs and collaborations throughout much of the country. Palliative care is cited as an essential health service in the Ugandan National Health Plan and prioritized by the government in multiple reports,[4] but financial constraints mean that funding for palliative care is still highly dependent on extramural donors.[5]

Figure 1. Examinations room.
According to statistics HAU compiled in 2016, an estimated 57% of Ugandans do not have access to health care6 and some 250,000 are in need of palliative care to improve their quality of life. Legislative efforts to broaden morphine-prescribing abilities to palliative care nurses and clinical officers have increased the availability of symptom relief in rural communities.[4] However, drug supplies are frequently limited.[7] In a survey of governmentfunded HIV care facilities in Kenya and Uganda, morphine was only intermittently available in 7% of facilities, whereas nonopioid adjuvant agents were available in 73% of facilities.[8] HAU opened a morphine sulfate–processing production in an attempt to address the limited opioid availability and is now the only manufacturer of morphine in the country.[9] Studies of selected patients in Kenya and Uganda suggest that patients diagnosed with cancer in this region experience a high burden of symptoms (a mean of 18 reported physical and psychological symptoms over the course of 7 days), with pain as the predominant complaint.[10] An estimated 46% of patients admitted to hospitals in Uganda had a life-limiting disease (vs estimates of 5–23% in comparable European studies). When interviewed, patients expressed concerns across multiple dimensions, including inability to afford medical care (50%) and limited access to food (14%), in addition to ofteninadequate symptom relief.[11]

Figure 2. Hospice complex.
HAU is the main referral site for all outpatient palliative care in the Kampala area and accommodates roughly 800 new patients per year. In total, 58% of the patients who present to HAU have cancer, most commonly cervical cancer (38%), followed by cancers of the breast (18%), esophagus (16%), or prostate (13%). Among HAU's patients, 9% present with comorbid HIV and cancer, and 21% follow up for other symptoms and issues related to HIV.[12] Only 12% of patients at HAU have a primary diagnosis that is not cancer or HIV. This subgroup includes patients with autoimmune disease as well as chronic pain; both conditions have limited treatment pathways. Patients frequently present with advanced malignancy and are subsequently referred for hospice management. For example, one patient sought care after her right breast had auto-amputated from necrotizing cancer. Other patients present with HIV-associated neuropathy or with a debilitating lower-extremity pain syndrome associated with AIDS.[13]
Patients treated at HAU receive multimodal analgesia in the form of morphine and nonopioid adjuvants, as well as wound care and medical supplies in exchange for a small donation. Roughly one-third of patients who are seen at HAU can afford to pay the fee (less than $3 USD), whereas the remainder receive charity care. Clinic hours are held daily and complemented by a home visit and outreach programs. HAU also trains community volunteers and offers palliative care courses for health care workers in other African countries.
In June 2017, I travelled to Kampala, Uganda, to work with HAU as part of my palliative medicine fellowship. I traveled with the hospice staff and saw patients in multiple care settings (Figures 1 and 2). Many of our patients were locals, others had travelled to Kampala for cancer evaluations not available in their home districts, and some were refugees. I took care of a 7-year-old child presenting with AIDS and severe abdominal pain because of bulky lymphadenopathy, a 10-year-old child with a hepatic mass and massive ascites, a woman who sustained extensive third-degree burns to her face and chest wall after seizing and falling into a cookfire, and another young woman who had just undergone hip disarticulation for hemangiopericytoma. All of these patients received pharmacologic pain management in addition to psychosocial counseling. HAU also offered a small stipend for additional care costs for families that were financially struggling.

Figure 3. Morphine supply under lock and key at a community hospital near Mbarara.
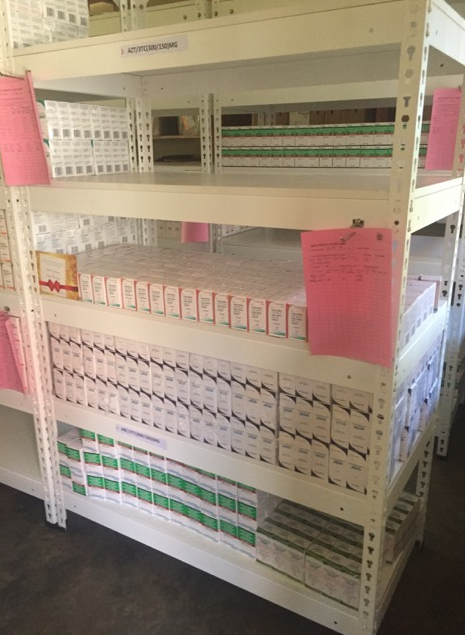
Figure 4: Stock of donated antiretrovirals at a community hospital.
Although the resources and pharmacy supplies at HAU may be small (Figures 3 and 4), the institution offers a distinct vision of multimodal symptom management. In spite of limited resources and training, the staff takes a comprehensive approach to patient care, which has had a substantive impact on the lives of over 28,000 patients to date.
References
- Kiwanuka JK, Ttendo SS, Eromo E, et al. Synchronous distance anesthesia education by Internet videoconference between Uganda and the United States. J Clin Anesth. 2015;27(6):499–503.
- Linden AF, Sekkide FS, Galukande M, Knowlton LM, Chackungal S, McQueen KAK. Challenges of surgery in developing countries: a survey of surgical and anesthesia capacity in Uganda's public hospitals. World J Surg. 2012;36:1056– 1065.
- LeBrun DG, Chackungal S, Chao TE, et al. Prioritizing essential surgery and safe anesthesia for the post-2015 development agenda: operative capacities of 78 district hospitals in 7 low- and middle-income countries. Surgery. 2014;155:365–373.
- Jagwe J, Merriman A. Uganda: delivering analgesia in rural Africa: opioid availability and nurse prescribing. J Pain Symptom Manage. 2007;33:547–551.
- Clark D, Wright M, Hunt J, Lynch T. Hospice and palliative care development in Africa: a multi-method review of services and experiences. J Pain Symptom Manage. 2007;33:698–710.
- Hospice Africa Uganda. 23rd annual report 2015–2016. Available at: http://www. annemerrimanfoundation.org/wp-content/uploads/2017/04/Annual-reportonine- version.pdf. Accessed November 30, 2017.
- Cleary J, Powell RA, Munene G, et al. Formulary availability and regulatory barriers to accessibility of opioids for cancer pain in Africa: report from the Global Opioid Policy Initiative (GOPI). Ann Oncol. 2013;24:xi14–xi23.
- Harding R, Simms V, Penfold S, et al. Availability of essential drugs for managing HIV-related pain and symptoms within 120 PEPFAR-funded health facilities in East Africa: a cross-sectional study with onsite verification. Palliat Med. 2014;28:293–301.
- Merriman A, Harding R. Pain control in the African context: the Ugandan introduction of affordable morphine to relieve suffering at the end of life. Philos Ethics Humanit Med. 2010;5:10.
- Harding R, Selman L, Agupio G, et al. The prevalence and burden of symptoms amongst cancer patients attending palliative care in two African countries. Eur J Cancer. 2011;47:51–56.
- Lewington J, Namukwaya E, Limoges J, Leng M, Harding R. Provision of palliative care for life-limiting disease in a low income country national hospital setting: how much is needed? BMJ Support Palliat Care. 2012;2:140–144.
- Hospice Africa Uganda. Fact sheet October 2016. Available at: http://www. friendsofhospiceafricausa.org/wp-content/uploads/2017/03/Finall-for-Oct16. pdf. Accessed November 30, 2017. 13. Norval DA. Symptoms and sites of pain experienced by AIDS patients. S Afr Med J. 2004;94:450–454.
Leave a commentOrder by
Newest on top Oldest on top