How I Do It: Botulinum Toxin for Cervical Dystonia
Cite as: Shah S. How I do it: botulinum toxin for cervical dystonia. ASRA News 2020;45. https://doi.org/10.52211/asra110120.068
While some postures of cervical dystonia are very visible, some complex features may lead to delayed diagnosis and treatment due to difficulty in identification.[1,2] In this article, I hope to clarify the mystery in appropriate diagnosis of the correct type of cervical dystonia postures as well as share botulinum toxin injection treatment pearls to correct these rotational postures. Visuals are key to understanding dystonia, so I attempted to place as many illustrations to help guide the reader with correct posture diagnosis and muscle identification.
Let the symptoms and patient’s goals be your driver in terms of which muscles to inject and the appropriate dose.
According to a study evaluating characteristics in 300 patients with cervical dystonia, approximately 66% of patients present with a combination of postures.[3] The importance of knowing and having a thorough understanding of these postures and terminologies to provide the correct treatment to the appropriate laterality of muscle groups cannot be overstated.
The four most common postures of cervical dystonia are (Figure 1):
- Torticollis: (rotated) 82% of patients
- Laterocollis: (to the side) 42% of patients
- Retrocollis (backward) 29%
- Anterocollis: (forward) 25% of patients
REMEMBER: 66% of patient will present with a COMBINATION of postures.[3]
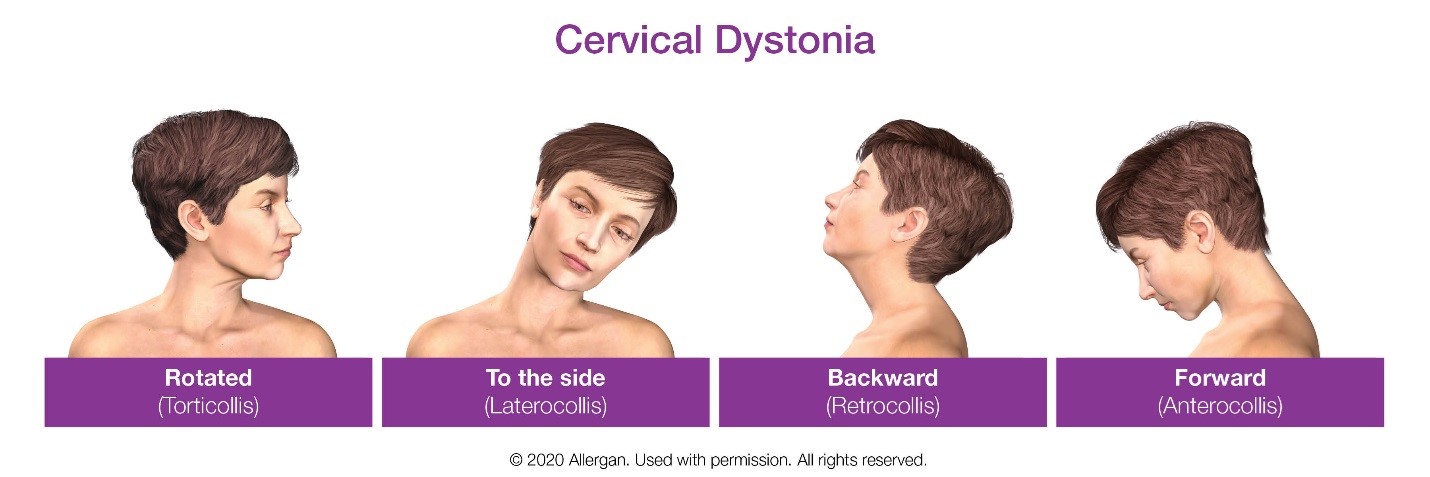
Figure 1: Common postures of cervical dystonia
The largest observational study of cervical dystonia (n= 1037) demonstrated that from time of onset of symptoms to diagnosis was a mean of 5 years and an additional mean of 1.2 years from diagnosis to any treatment. (1,2). 89% of patients will present with neck pain and 66% will have a head tremor. Commonly mistaken differential diagnoses include cervical spondylosis, myofascial pain or Parkinson’s.[4]
While the focus of this article is more about injection techniques, I wanted to share a great reference article by Consky et al., which may aid in understanding cervical dystonia more thoroughly.[5] Figure 2 demonstrates the muscles commonly involved in cervical dystonia.
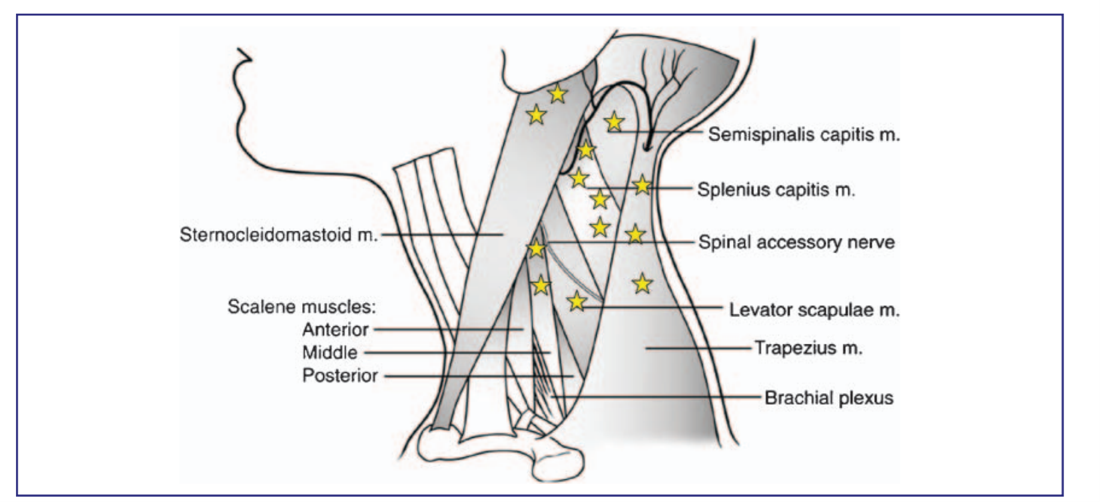
Figure 2: Neck muscles involved in cervical dystonia[6]
Muscle Identification
Let’s begin with the most commonly seen posture, torticollis.
In torticollis, there are contralateral and ipsilateral muscles to identify and inject. This is the only posture that requires you to understand contra vs ipsi injections. Ipsilateral is defined as the same side as the rotational direction of the patient’s head. Figure 3 represents the clinical presentation of contralateral versus ipsilateral muscle involvement. In Figure 3, ipsilateral is the patient’s left.
- Ipsilateral
- Splenius capitus
- Levator scapulae
- Longissimis
- Rectus capitus posterior major (not approved)
- Obliquus capitus (not approved)
- Contralateral
- Sternocleidomastoid
- Upper trapezius
- Scalene anterior
- Semispinalis cervicis (not approved for toxin injection)
- Multifidus (not approved for toxin injection)
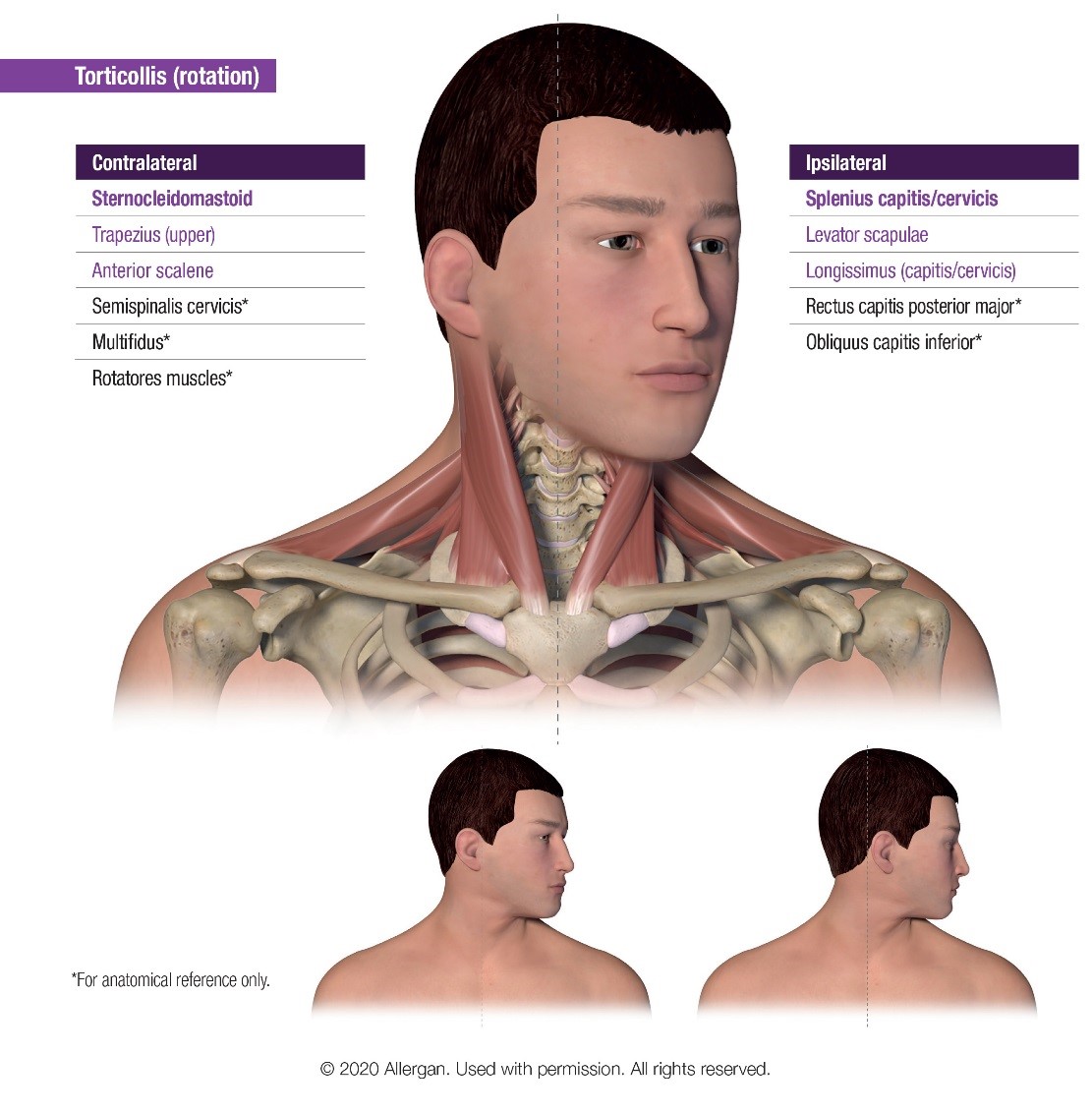
Figure 3: Clinical presentation of torticollis contralateral versus ipsilateral muscles
Laterocollis: Ipsilateral injection ONLY!
In laterocollis, the following muscles are injected ipsilaterally. Note the characteristic of the posture is a tilt, rather than a rotation.
- Levator scapulae
- Upper trapezius
- Scalene (anterior, middle, and posterior)
- Sternocleidomastoid
- Splenius capitus
- Splenius cervicis
- Longissimus
- Multifidus (not approved for injection)
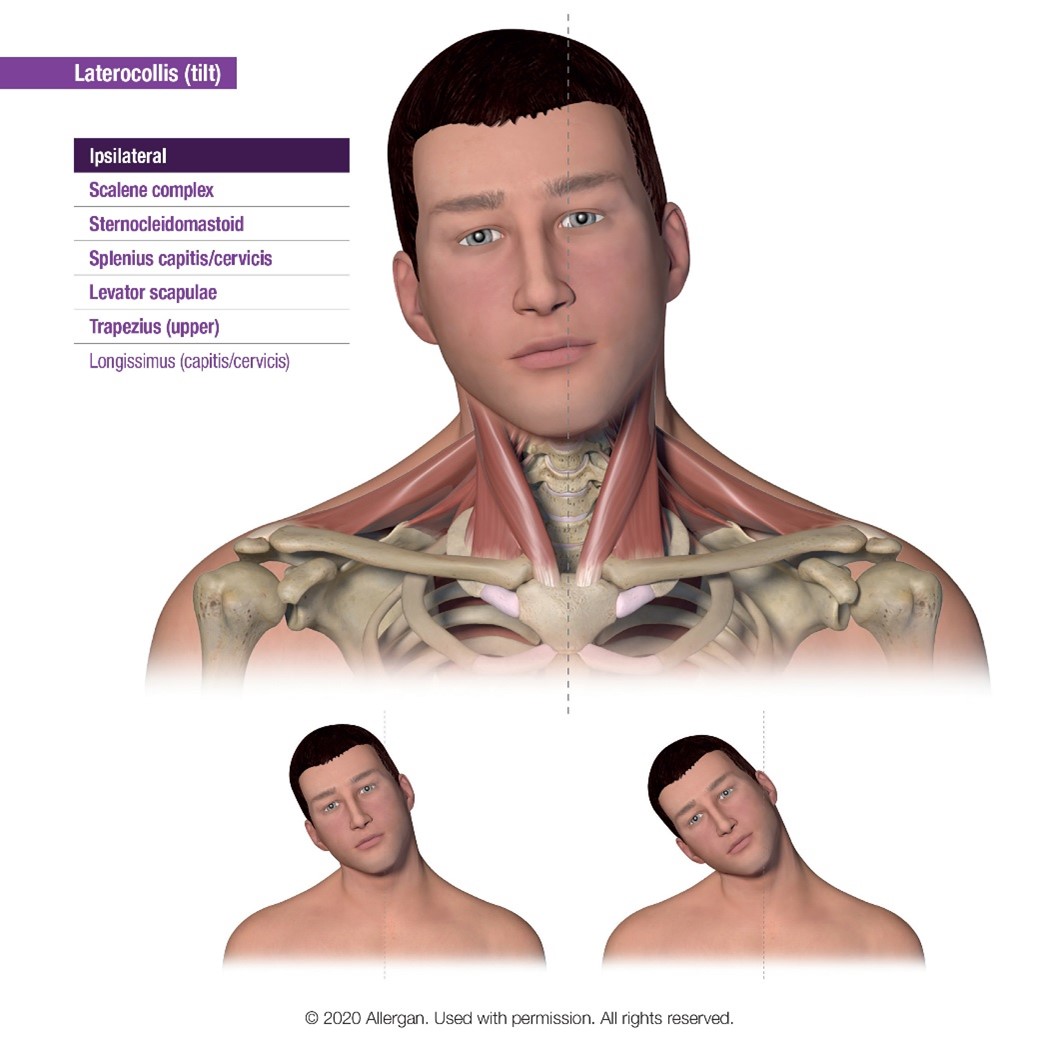
Figure 4: Laterocollis muscle involvement
Anterocollis: BILATERAL injections in symmetric muscle groups
While three major muscle groups are involved in anterocollis (scalene complex, longus capitus, rectus capitus), only one complex is approved for toxin injection (scalene complex).
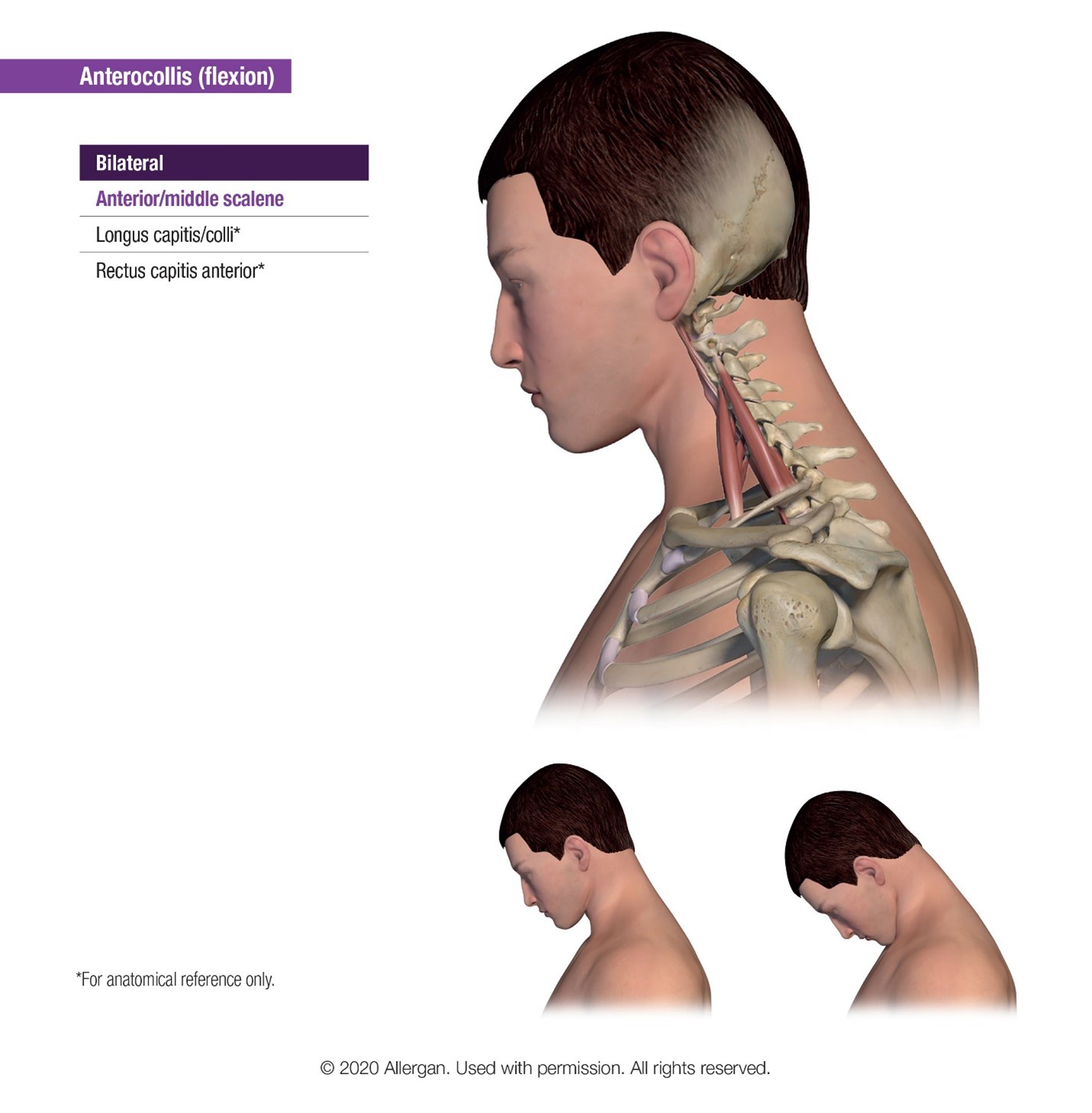
Figure 5: Anterocollis muscles involvement
Retrocollis: This extension posture requires BILATERAL SYMMETRIC injection in the following muscle beds:
- Levator scapulae
- Upper trapezius
- Longissimus
- Splenius capitus
- Splenius cervicis
- Semispinalis capitus
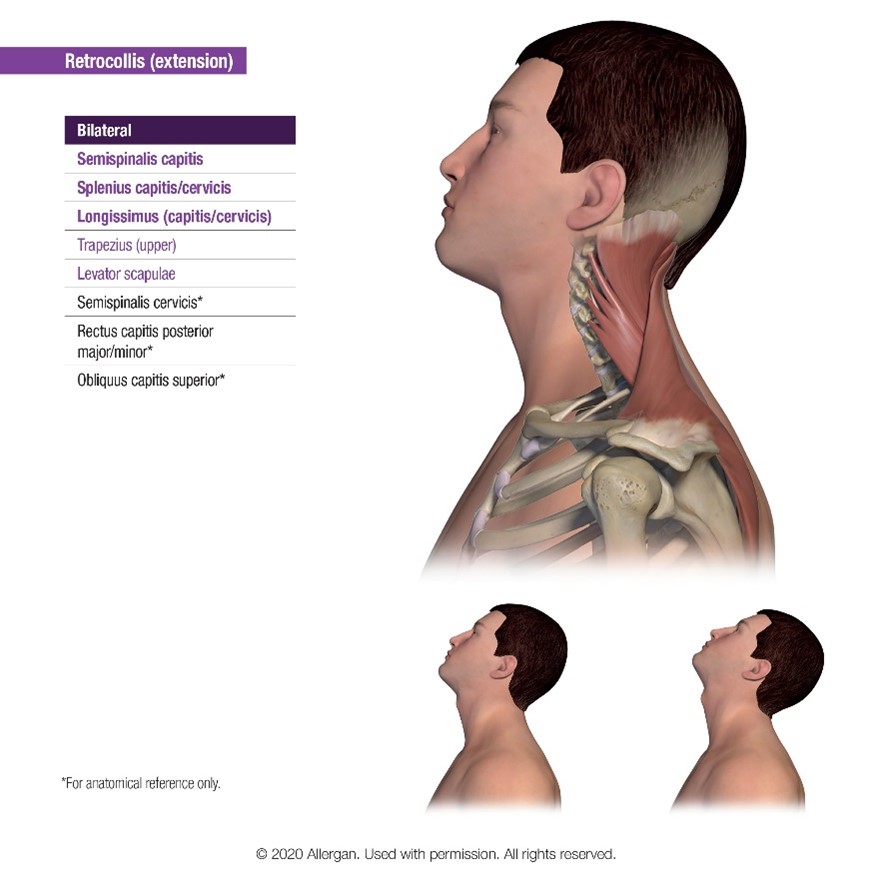
Figure 6: Retrocollis muscle involvement and posturing
As you may have noticed, several muscle groups are identified as injection targets for all or many of the above postures. Therefore, we will focus on injection pearls for the most commonly injected muscle targets.
Sternocleidomastoid: This muscle unilaterally tilts the head ipsilaterally and rotates contralaterally. It also extends the head and pulls the neck forward. Therefore it is a target in anterocollis, laterocollis, and torticollis. This muscle can be localized with contralateral rotation of the head. Note that you may find the sternocleidomastoid is quite hypertrophied in patients with contralateral torticollis. Recommended injection dose of 15-100 units.
Upper trapezius: This muscle unilaterally rotates the head to the opposite side and bilaterally extends the head. The postures that involve the upper trapezius include laterocollis, retrocollis, and torticollis. Isolate the trapezius at 2 fingerbreadths below the nuchal line at a depth of 1cm; recommended injection dose is 20-100 units.
The scalene complex unilaterally bends the neck to the same side, and is made up of the anterior, medius, and posterior muscles. One may consider using ultrasound for this muscle injection to avoid contacting the brachial plexus. Recommended injection is 15-50 units.
Conclusion and Guiding Principles
As an overall framework, the first step in treating cervical dystonia with botulinum toxin therapy is to identify which posture your patient presents with, appreciating that approximately two-thirds of patients with dystonia will have more than one posture. Let the symptoms and patient’s goals be your driver in terms of which muscles to inject and the appropriate dose. The muscle injected and the doses may need to be adjusted during subsequent injection sessions. Caution should be taken as aggressive dosing may cause head lag, dysphonia, and swallowing difficulties. Overall, treating cervical dystonia effectively with botulinum toxin is extremely rewarding. It will allow you to appreciate improvement in the rotational aspects of the patient’s dystonia, improvement in pain symptomology, and a definitive improvement in their quality of life.
References
- Stacy M. Epidemiology, clinical presentation, and diagnosis of cervical dystonia. Neurol Clin. 2008; 26(suppl 1):23-42.
- Tiderington E, Goodman EM, Rosen AR, et al. How long does it take to diagnose cervical dystonia?J. Neurol Sci 2013;335 (1-2):72-4.
- Jankovic J, Leder S, Warner D, Schwartz K. Cervical dystonia: clinical findings and associated movement disorders. 1991;41(7):1088-91.
- Bhidayasiri R, Kaewwilai L, Wannachai N, et al. Prevalence and diagnostic challenge of dystonia in Thailand: a service-based study in a tertiary university referral centre. Parkinsonism Relat Disord.2011;17(Suppl. 1):S15-S9.
- Consky ES, Lang AE. Clinical assessments of patients with cervical dystonia. In: Jankovic J, Hallet M (eds.). Therapy with Botulinum Toxin. New York, NY: Marcel Dekker, Inc; 1994.
- Kamm C, Benecke R. Individualized management of cervical dystonia with different serotypes of botulinum toxin: recent therapeutic advances and risk of development of neutralizing antibodies. Eur Neurol J. 2010;2:49-54.
Leave a commentOrder by
Newest on top Oldest on top