How I Do It: The Vertiflex® Procedure for Lumbar Spinal Stenosis
Cite as: Weisbein J. How I do it: the Vertiflex® procedure for lumbar spinal stenosis. ASRA News 2020;45. https://doi.org/10.52211/asra110120.073
One of the most common indications for spinal surgery in patients over 65 years of age is lumbar spinal stenosis with associated neurogenic claudication. The diagnosis includes clinical manifestations of low back pain with associated lower extremity paresthesia or neurologic manifestations coupled with imaging findings consistent with narrowing of the central canal, the lateral recesses, or neuroforamina.[1] Treatment options from a conservative standpoint can be limited; however, research in the surgical field has led to improvements in minimally invasive surgical techniques.[2] These can be extremely beneficial for patients with medical comorbidities that might prohibit them from undergoing open surgical techniques.[3]
These can be extremely beneficial for patients with medical comorbidities that might prohibit them from undergoing open surgical techniques
The Superion Indirect Decompression System is indicated for treatment of patients with neurogenic claudication from moderate degenerative lumbar spinal stenosis, in a stable spine, with no greater than a grade 1 spondylolisthesis. Patients who can relieve their symptoms with flexion or sitting down are the best candidates for this procedure. Other anatomical considerations that might preclude a patient from being an appropriate candidate for this procedure include thin spinous processes, “kissing spine,” and short spinous processes that will make placement of the implant too shallow.[4] Unlike open procedures, VertiflexTM does not require the resection of any anatomical structures, can be completed in an outpatient setting without the need for general anesthesia, and is completely reversible.

Figure 1. The device is implanted with a provided sterile tool kit.
Used with permission from BSCI
With any interventional procedure, appropriate patient positioning is a vital step for success. The patient should be positioned prone on a radiolucent table with bolsters under the abdomen to adequately flex the lumbar spine. This allows for the separation of the spinous processes to introduce the device. Under fluoroscopic guidance, the level to be treated should be identified and marked. After adequate local anesthesia, an incision approximately half an inch in length is made in the midline and is taken down to the depth of the supraspinous ligament. This is performed under anteroposterior (AP) and lateral fluoroscopic projections. The dilator assembly (Figure 1A) is placed midline and advanced with the use of a mallet until the distal tip is close to the dorsal aspect of the facet shadow or spinolaminar junction. The dilator assembly should be placed midline, between the spinal process above and the spinal process below. The dilator assembly is unlocked, and the cannula assembly (Figure 1B) placed over it. It is imperative to advance the cannula assembly carefully, taking precautions to not further advance the dilator and ensure the trajectory stays midline. This is verified by depth in the lateral view, and then frequently checking the AP view and adjusting the cranial-caudal position of the cannula on the spinous processes. The distal tip of the cannula assembly should reach the spinolaminar junction while the distal end is positioned beyond the tips of the spinal processes. Inappropriate placement of the cannula assembly will prohibit the device from properly being deployed or cause dural injury. Take the extra time to make sure the distal end of the cannula assembly is approximately 10mm dorsal to the spinolaminar junction.
After the cannula assembly is in the appropriate position, the supplied reamer (Figure 1C) is inserted through it in a lateral fluoroscopic view, with careful precautions to not advance the reamer past the spinolaminar junction. The reamer should be turned clockwise and counterclockwise then removed.
The size of the implant to be used is determined by the interspinous gauge (Figure 1D). This device is inserted through the cannula. A measurement of the interspinous space is indicated on the instrument after gripping the device firmly until resistance is detected at the distal tip. The goal of sizing is not to distract spinous processes but to determine which implant will be inserted. It is recommended to downsize rather than upsize on the implant. While the interspinous gauge is deployed, the AP image should be checked with cranial-caudal adjustments to confirm that superior and inferior aspects of the distal tips are visualized and midline. The interspinous gauge is then removed.
Once the implant size is selected, it is loaded onto the inserter (Figure 1E) by aligning the arrow on the body of the Implant with the arrow on the end of the inserter. The lever is flipped down to lock the implant into place. The driver (Figure 1F) is placed through the inserter and rotated to engage the implant. The implant is deployed under lateral fluoroscopic view. Do not rotate the driver without checking for proper positioning at frequent intervals. This could result in fracture of the driver edge or malalignment of the implant. Once the implant is slightly deployed, obtain an AP and cranial-caudad fluoroscopic image to ensure that the implant is being deployed with bilateral containment of the superior and inferior spinous processes.
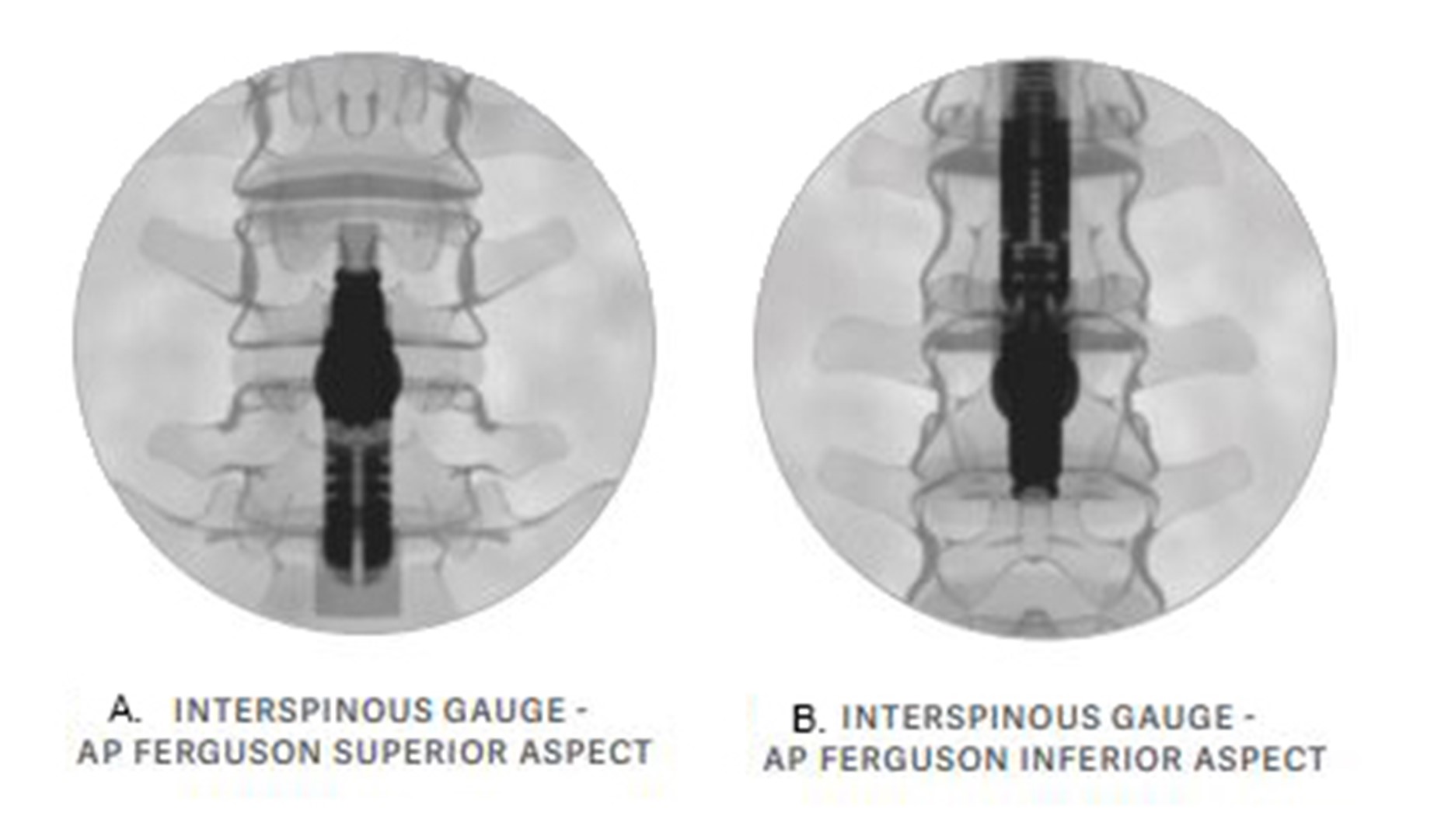
Figure 2. Cranial caudal adjustments of the C-Arm allow for A. superior spinous process and B. Inferior spinous process viewing of the device while being deployed. Used with permission from BSCI
If the alignment appears appropriate but resistance is encountered, rocking the inserter/driver cranial or caudal can assist in creating additional space to deploy the implant. This should be done under intermittent fluoroscopy in AP and lateral trajectories to make sure the device is properly deploying. When the implant is completely open, the driver is removed and gentle tapping with a mallet is used for final placement. The implant should not be left too shallow or dorsal for risk of spinous process fracture. Final positioning is confirmed by a lateral fluoroscopic view. An audible change in the sound emitted from tapping the inserter is also used to confirm final positioning. The lever on the inserter should be opened, and the inserter and cannula should be removed from the incision. After irrigation of the incision, a 3-0 Vicryl, 4-0 Monocryl, and topical skin adhesive can be used for closure.
Important things to consider:
- Two contiguous levels can be performed, but the most symptomatic level should be treated first to ensure adequate decompression.
- Do not deploy the dilator too deep. If it is too deep, you will have difficulty deploying the implant. Additionally, be precise and meticulous about your alignment.
- Ensuring throughout the procedure that your placement is optimal. This is going to allow for ease of deployment of the implant.
- Patients with scoliosis can be treated, but it is imperative that the Cobb angle at the level to be treated is no greater than 10 degrees.
- The interspinous gauge should not be over- or under-deployed, as oversizing can cause increased pain or fracture at the site and undersizing can inhibit adequate decompression of the targeted treatment level.
- Perioperative antibiotics should be administered like other implantable device.
- Patients who have undergone a fusion where adjacent levels above or below the fusion have developed symptomatic stenosis may still be candidates for this procedure. Additionally, patients with previously placed implantable devices like intrathecal pumps or spinal cord stimulators that have developed symptomatic lumbar stenosis also may be candidates. Avoid patients that have undergone a hemilaminectomy as the integrity of the spinous process is less and may predispose to fracture.
Removal of the device can be done either by an open procedure or under fluoroscopic guidance using the aforementioned dilation techniques. Once the inserter is locked in place, the driver is placed and gently rotated until it engages the implant. Continue to rotate counter-clockwise until the implant is completely disengaged from the spinal processes and can be withdrawn.
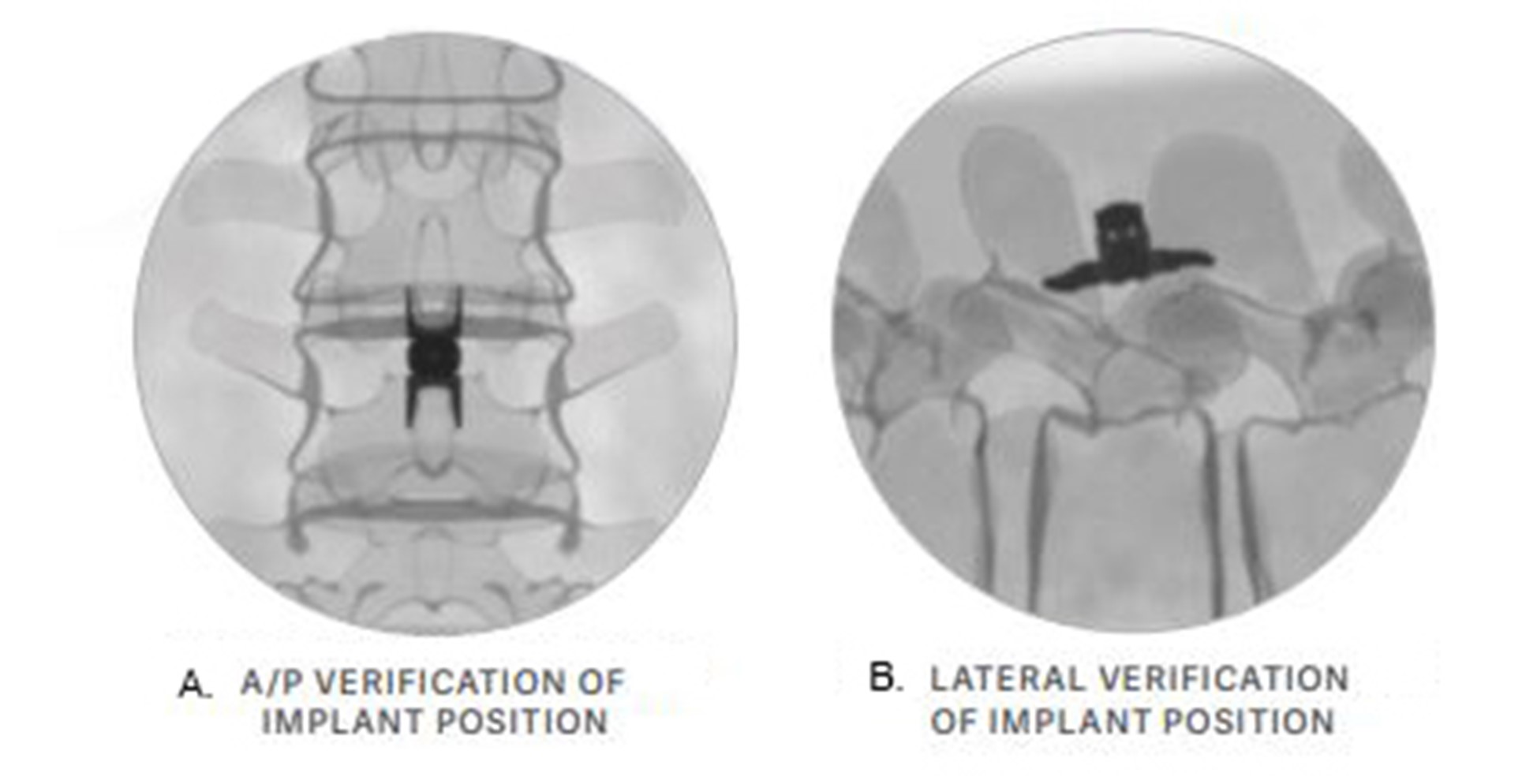
Figure 3. The optimal implant position can be seen here in the (A) A/P view and (B) lateral view. Used with permission from BSCI
The Superion Indirect Decompression System is a simple procedure that should only be performed by physicians who have received adequate training. With careful patient selection and attention to detail, patients can have relief from their symptoms of neurogenic claudication in under 15 minutes.
References
- Lurie J, Tomkins-Lane C. Management of lumbar spinal stenosis. BMJ. 2016;352:h6234.
- Zaina F, Tomkins-Lane C, Carragee E, Negrini S. Surgical versus non-surgical treatment for lumbar spinal stenosis. Cochrane Database Syst Rev. 2016;2016(1):CD010264. Published 2016 Jan 29. doi:10.1002/14651858.CD010264.pub2
- Hartman J, Granville M, Jacobson RE. The use of Vertiflex® interspinous spacer device in patients with lumbar spinal stenosis and concurrent medical comorbidities. Cureus. 2019;11(8):e5374.
- Boston Scientific. Vertiflex superion indirect decompression system: instructions for use. Valenica, CA; 2020.
Leave a commentOrder by
Newest on top Oldest on top