Working with Acute Pain Colleagues on Opioid Reduction in the Postsurgical Population
Cite as: Singla P, Renwick C, Kohan L, Yalamuru B. Working with acute pain colleagues on opioid reduction in the postsurgical population. ASRA Pain Medicine News 2022;47. https://doi.org/10.52211/asra110122.052
Introduction
Opioids have long been used for management of chronic pain conditions, often as a bridge until surgery, such as with chronic back or joint pain.1 About 1 in 4 patients who present for surgery are on preoperative opioids.2 This poses an enormous problem with providing safe and effective pain management in the perioperative setting should patients already have some degree of tolerance.
Rationale to Minimize Preoperative Opioids
Preoperative opioid usage has been associated with significantly higher subjective pain ratings and postoperative pain medication requirements, including opioid escalation.3-5 A survey of chronic pain providers found the prevalence of opioid induced hyperalgesia (OIH) to be at an average of 6.8 cases per practice year.6 In addition to OIH, preoperative opioid usage also leads to worse clinical outcomes, such as longer hospital stays and pulmonary complications (with odds ratios of 2.5 and 3.1, respectively).7 Patients who have used opioids chronically have an increased incidence of acute respiratory failure, prolonged mechanical ventilation, and reintubation8 due to their tolerance to the analgesic effects of opioids (leading to higher opioid dosages) but incomplete tolerance to the effects on respiratory depression. Even after discharge, the sequelae from chronic preoperative opioid usage can be seen with up to 77% of patients remaining on chronic opioids postoperatively and continuing to have refractory pain.9-10 Ultimately, this refractory pain leads patients to seek revisions or more invasive surgeries in the future.11
Identifying High Risk Patients for Postoperative Pain
Considering the poor outcomes following chronic preoperative opioid usage—including increased risk of morbidity, mortality, prolonged hospital stays, respiratory failure, prolonged mechanical ventilation, myocardial infarction, and postoperative ileus7—healthcare systems and clinicians have been attempting to reduce preoperative opioid usage. Once the decision has been made to reduce—and ideally avoid—preoperative opioid usage, the next challenge lies in identifying patients at greater risk for postoperative pain.
A survey of chronic pain providers found the prevalence of opioid induced hyperalgesia to be at an average of 6.8 cases per practice year.
Preoperative opioid usage is not the only risk factor for development of significant post-operative pain and difficulties. Other factors include any history of an opioid use disorder (regardless of medication for opioid use disorder), history of substance abuse (including alcohol and sedative/hypnotics), and history of neuropsychiatric disorders.12, 13 Additionally, the type of surgery itself can weigh heavily on anticipated postoperative pain and opioid requirements. By anatomic location, thoracic and spinal surgeries14 are routinely categorized as some of the more painful surgical interventions, and, for the latter, these patient populations often present to surgery with a history of chronic pain.
Mitigating Postoperative Pain in the Opioid Naïve Patient
The importance of adequate postoperative pain cannot be overemphasized. Most institutions have developed enhanced recovery after surgery (ERAS) pathways, with the goal of faster recovery and reduced postoperative opioid utilization. Multimodal analgesia is one of the most important pillars of any ERAS pathway.
Multimodal analgesia is defined as “the use of a variety of analgesic medication and techniques that target different mechanisms of action in the peripheral and/or central nervous system (which might also be combined with non-pharmacological interventions) might have additive or synergistic effects and more effective pain relief compared with single-modality interventions.”15 With the realization of harmful effects of opioid administration, there has been a paradigm shift to maximize utilization of nonopioid medications. Regional anesthesia techniques are one of the most effective components of opioid-sparing analgesia.
Role of the Acute Pain Service in Management of Postoperative Pain
Acute pain service (APS) is a unique perioperative pain management specialty16 that provides individualized approaches to pain management. The goal is to reduce over-reliance on opioids17 and, at the same time, educate patients about the perils of inadequate pain control and the consequences of persistent opioid use and substance use disorders. The current ERAS guidelines have been adopted widely and help with postoperative pain control. However, due to presence of comorbidities as well as preexisting medication use, APS can help choose and modify the optimal technique that would provide maximal benefit for pain relief and minimize side effects.
Management of acute pain starts with a comprehensive preoperative evaluation of the patient’s preexisting chronic pain and medications, along with any medical and psychological comorbidities (cardiac or respiratory issues, current use of anticoagulants, opioid use disorder etc.)15,18 as previously alluded to.
A major area of focus of the APS team is immediate postoperative inpatient care,10 which is probably the most vulnerable period in terms of pain control. Inadequate pain control can lead to chronic post-surgical pain (CPSP). The incidence of CPSP varies by the type of surgery14, 19, 20 and can be as high as 10%.21, 22 CPSP has enormous implications for society by adding substantial amounts to the cost of healthcare.19 On an individual level, CPSP has found to be a prominent factor for persistent opioid use that predisposes patients to increased morbidity from the adverse effects of opioids and opioid use disorder. It also was found to be associated with low mood and reduced function.20, 22
ERAS pathways lay the foundation for pain control; however, one size does not fit all. The postoperative analgesia plan must be individualized, based on preoperative assessment with adjustment based on constant postoperative reassessment. APS is an ideal team for this purpose. APS providers are very well versed in medication management as well as rescue regional anesthesia techniques. APS providers are generally pain physicians or anesthesiologists who have comprehensive training in managing pain with medications, including opioids, non-opioid adjuncts, and regional anesthesia techniques, as well as conservative measures.
A recent trend toward transitional perioperative pain services broadens the horizon and addresses fragmentation of comprehensive perioperative pain management.18, 23 There is increasing recognition of the burden of untreated postoperative pain after discharge and, hence, the need for long-term follow up and treatment of patients who develop or are at risk of developing persistent postsurgical pain. Patients on preoperative opioids commonly leave the hospital with substantial increases in opioid dose from baseline without an appropriate weaning plan.22 APS typically helps with immediate postoperative pain control while the patient is in the hospital. Transitional pain teams, on the other hand, are unique as they help with preoperative planning and weaning of medications, immediate postoperative pain management, and outpatient follow up and pain management after surgery.22 Transitional pain teams have been successful in reducing overall opioid use by closely monitoring patients in the acute postoperative phase, inpatient as well as after discharge, and intervening appropriately to modify the treatment strategies in patients who are not recovering appropriately.18,22,23
How We Do It at the University of Virginia
At the University of Virginia (UVA), we use a hybrid model, which entails a concurrent operating room regional anesthesia team for preoperative regional anesthesia procedures as well as a stand-alone APS team. Figure 1 shows the organization of the APS team at UVA.
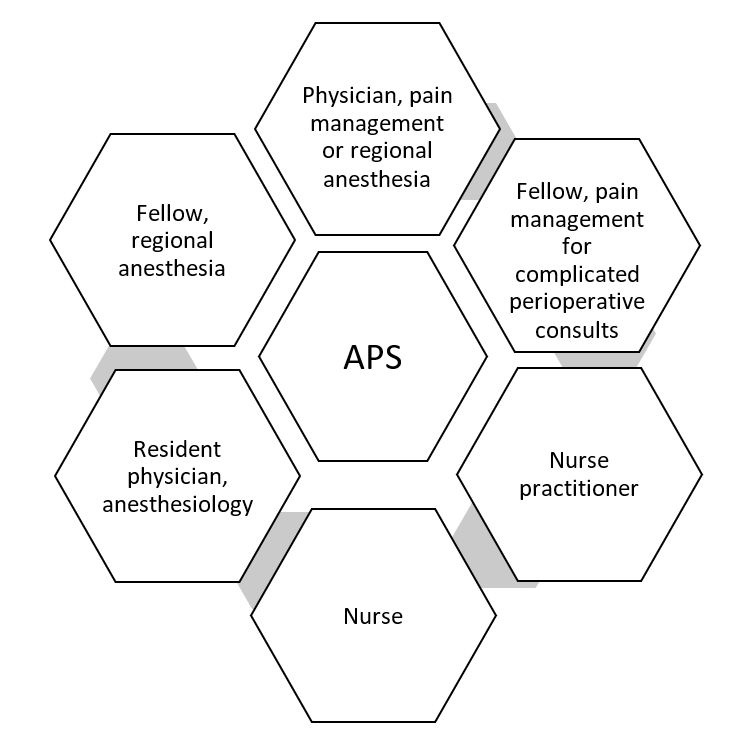
Figure 1. Acute Pain Service Organization at the University of Virginia
We have initiated a perioperative program based on the seven principles18 of the acute perioperative pain management for patients at high risk of postoperative pain. Once the surgeon or our anesthesia preoperative assessment clinic identifies these patients, our pain medicine specialists assess them to formulate a multimodal, comprehensive, and individualized plan.
For most of the patients on chronic preoperative opioid medications, this is a collaborative effort, which includes input from the patient's primary care provider or pain physician, our acute pain team physician, and our chronic pain physicians. Patients are encouraged to wean opioids preoperatively, starting with the extended release or long-acting forms first. Preoperative interventions include performing appropriate interventional pain procedures to optimize coexisting pain not related to surgical procedure. For example, medial branch blocks and radiofrequency ablation can be performed for patients who have facet mediated axial back pain and are taking opioids for the same but are scheduled to undergo knee replacement. This might help to wean opioids before the knee surgery.
Our APS team coordinates with the anesthesia team regarding the intraoperative analgesia plan. We have multiple ERAS pathways tailored to various surgeries. Regional and neuraxial catheters are used as appropriate. Postoperative opioid use is minimized by use of adjuvants such as acetaminophen, nonsteroidal anti-inflammatory agents, muscle relaxants, and continuous infusions of lidocaine (if the patient is not a candidate for nerve block or catheter using local anesthetics) and/or ketamine. The APS team follows patients until discharge for assessment of pain control as well as employing rescue techniques such as postoperative peripheral nerve catheters, fascial plane blocks, etc., as needed.
After the patient is discharged home, our pain management physicians follow up for up to 90 days for continued postoperative pain management.
Our team at UVA is a collaborative effort between various specialties. Figure 2 shows the various teams that APS works with at UVA for perioperative pain management. We have been able to integrate the translational and APS teams to a certain extent.
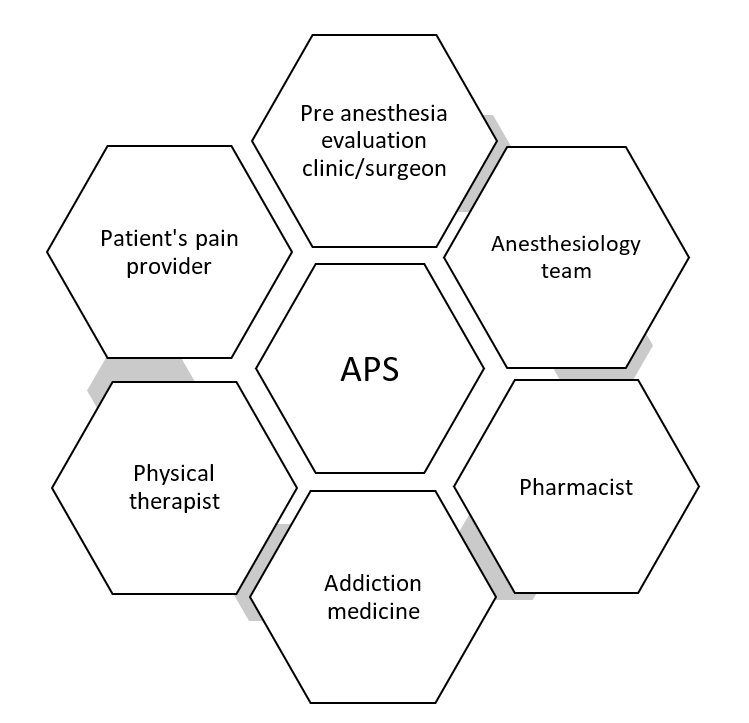
Figure 2. Collaborating Teams Within the APS at the University of Virginia
Conclusion
The importance of controlling acute postoperative pain cannot be overemphasized. APS plays a pivotal role in this regard. The joint effort of pain management physicians as well as acute pain physicians aims to manage the postoperative analgesic needs of the patient better than the teams working in silos. This is especially true in patients with a history of chronic pain and those on long-term opioids or neuropathic agents undergoing surgery. We have found that having a cohesive and collaborative team of physicians, nurses, and other healthcare personnel in the perioperative period to manage acute postoperative pain improves the patients’ experience and outcomes.
Priyanka Singla, MD is an assistant professor in the department of anesthesiology at the University of Virginia in Charlottesville.
Christian Renwick is a medical student at the University of Virginia School of Medicine in Charlottesville.

Lynn Kohan, MD, is a professor of anesthesiology and the program director of the pain medicine fellowship at the University of Virginia in Charlottesville.
Bhavana Yalamuru, MD, is an assistant professor in the department of anesthesiology at the University of Virginia in Charlottesville.
References
- De Sola H, Dueñas M, Salazar A, et al. Prevalence of therapeutic use of opioids in chronic non-cancer pain patients and associated factors: a systematic review and meta-analysis. Frontiers in Pharmacology 2020;11. https://doi.org/10.3389/fphar.2020.564412
- Hilliard PE, Waljee J, Moser S, et al. Prevalence of preoperative opioid use and characteristics associated with opioid use among patients presenting for surgery. JAMA Surg 2018;153(10):929–37. https://doi.org/10.1001/jamasurg.2018.2102
- Armaghani SJ, Lee DS, Bible JE, et al. Preoperative opioid use and its association with perioperative opioid demand and postoperative opioid independence in patients undergoing spine surgery. Spine 2014; 39(25):E1524. https://doi.org/10.1097/BRS.0000000000000622
- Goplen CM, Verbeek W, Kang SH, et al. Preoperative opioid use is associated with worse patient outcomes after total joint arthroplasty: a systematic review and meta-analysis. BMC Musculoskeletal Disorders 2019;20(1):234. https://doi.org/10.1186/s12891-019-2619-8
- Smith SR, Bido J, Collins JE, Yang H, et al. Impact of preoperative opioid use on total knee arthroplasty outcomes. J Bone Joint Surg Am 2017;99(10):803-8. https://doi.org/10.2106/JBJS.16.01200
- Vargas-Schaffer G, Paquet S, Neron A, et al. Opioid induced hyperalgesia, a research phenomenon or a clinical reality? results of a Canadian Survey. J Pers Med 2020;10(2):27. https://doi.org/10.3390/jpm10020027
- Menendez ME, Ring D, Bateman BT. Preoperative opioid misuse is associated with increased morbidity and mortality after elective orthopaedic surgery. Clinical Orthopaed Rel Res 2015;473(7):2402-12. https://doi.org/10.1007/s11999-015-4173-5
- Sayal P, Bateman BT, Menendez M, et al. Opioid use disorders and the risk of postoperative pulmonary complications. Anesth Analg 2018;127(3):767-74. https://doi.org/10.1213/ANE.0000000000003307
- Raebel MA, Newcomer SR, Reifler LM, et al. Chronic use of opioid medications before and after bariatric surgery. JAMA 2013;310(13):1369. https://doi.org/10.1001/jama.2013.278344
- Hanna MN, Speed TJ, Shechter R, et al. An innovative perioperative pain program for chronic opioid users: an academic medical center’s response to the opioid crisis. Am J Med Qual 2019;34(1):5-13. https://doi.org/10.1177/1062860618777298
- Ben-Ari A, Chansky H, Rozet I. Preoperative opioid use is associated with early revision after total knee arthroplasty: a study of male patients treated in the Veterans Affairs System. JBJS 2017;99(1):1-9. https://doi.org/10.2106/JBJS.16.00167
- Ward EN, Quaye ANA, Wilens TE. Opioid use disorders: perioperative management of a special population. Anesth Analg 2018;127(2):539-47. https://doi.org/10.1213/ANE.0000000000003477
- Burcher KM, Suprun A, Smith A. Risk factors for opioid use disorders in adult postsurgical patients. Cureus 2018;10(5). https://doi.org/10.7759/cureus.2611
- Zhao S, Chen F, Feng A, et al. Risk factors and prevention strategies for postoperative opioid abuse. Pain Res Manag 2019;2019:e7490801. https://doi.org/10.1155/2019/7490801
- Chou R, Gordon DB, de Leon-Casasola OA, et al. Management of postoperative pain: a clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists' Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain 2016 Feb; 17(2):131-57. https://doi.org/10.1016/j.jpain.2015.12.008
- Missair A, Visan A, Ivie R, et al. Daring discourse: should acute pain medicine be a stand-alone service? Reg Anesth Pain Med 2021 Jun; 46(6):529-31. https://doi.org/10.1136/rapm-2020-102288
- Cheng J, Rutherford M, Singh VM. The HHS Pain Management Best Practice Inter-Agency Task Force report calls for patient-centered and individualized care. Pain Med 2020; 21(1):1-3. https://doi.org/10.1093/pm/pnz303
- Mariano ER, Dickerson DM, Szokol JW, et al. A multisociety organizational consensus process to define guiding principles for acute perioperative pain management. Reg Anesth Pain Med 2022;47(2):118-27. https://doi.org/10.1136/rapm-2021-103083
- Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res 2017;10:2287-98. https://doi.org/10.2147/JPR.S144066
- Huang A, Azam A, Segal S, et al. Chronic postsurgical pain and persistent opioid use following surgery: the need for a transitional pain service. Pain Manag 2016;6(5):435-43. https://doi.org/10.2217/pmt-2016-0004
- Glare P, Aubrey KR, Myles PS. Transition from acute to chronic pain after surgery. Lancet 2019;393(10180):1537-46. https://doi.org/10.1016/S0140-6736(19)30352-6
- Clarke H. Transitional pain medicine: novel pharmacological treatments for the management of moderate to severe postsurgical pain. Expert Rev Clin Pharmacol 2016;9(3):345-9. https://doi.org/10.1586/17512433.2016
- Buys MJ, Bayless K, Romesser J, et al. Opioid use among veterans undergoing major joint surgery managed by a multidisciplinary transitional pain service. Reg Anesth Pain Med 2020 Nov;45(11):847-52. https://doi.org/10.1136/rapm-2020-101797