PECS I and PECS II Blocks
Author
Jaime Ortiz, MD
Associate Professor of Anesthesiology
Director of Regional Anesthesia
Co-Director of Acute Pain Management Service
Baylor College of Medicine
Houston, TX
Indications
PECS blocks were first described by Blanco[1-2] in 2011. A PECS block is a fascial plane block that provides analgesia to the upper anterior chest wall. It has been used for analgesia after breast surgery. [1-3] It has also shown potential to provide analgesia for pacemaker insertion[4] and upper arm fistula surgery.[5] It is an alternative to paravertebral blocks in patients receiving breast surgery.
Anatomy
The PECS I block targets the pectoral nerves, which arise from the brachial plexus cords. The lateral pectoral nerve arises from C5-7, runs between the pectoralis major and minor muscles, and supplies innervation to the pectoralis major muscle. The medial pectoral nerve arises from C8-T1, runs deep to the pectoralis minor, and innervates the pectoralis major and minor muscles. The PECS I block will block the lateral and medial pectoral nerves and is useful for surgeries involving the pectoralis major muscle, such as breast expander, subpectoral prosthesis, pacemaker insertion, and portacath placement.
The PECS II block targets the anterior and lateral divisions of the thoracic intercostal nerves T2-6, which run in a place between intercostal muscles. In addition, the PECS II block provides analgesia of the long thoracic nerve, which arises from C5-7 and innervates the serratus anterior muscle, and the thoracodorsal nerve, which arises from C6-8 and innervates the latissimus dorsi muscle. The PECS II block is used when patients are receiving more extensive breast surgery such as tumor resection and mastectomy, involving the pectoralis major and minor muscles, the serratus anterior muscle, and the axilla.
Equipment
- Ultrasound machine with linear transducer (6-13 MHz), sterile sleeve, and gel
- Standard nerve block tray
- Two 10-20-mL syringes for the local anesthetic
- 50- to 100-mm, 20- to 22-gauge insulated needle
- 2% chlorhexidine preps
- Sterile gloves, cap, mask
- Standard ASA monitors, IV access
- Oxygen by nasal cannula
- Drugs for sedation (midazolam, fentanyl)
Drugs
Sedation
- 1-2 mg midazolam, as needed
- 50-100 mcg fentanyl, as needed
Local anesthetics
- Mepivacaine 1.5%
- Bupivacaine 0.25%
- Ropivacaine 0.5%
Technique
The technique was initially described by Blanco.[1-2] The patient is placed in the supine position with the arm abducted. A high-frequency ultrasound probe is placed under the clavicle at the midclavicular line to locate the axillary artery and vein under the pectoralis major and minor muscles. The probe is then moved distally and laterally towards the axilla as you visualize the ribs. Starting at the 1st rib, count until you reach the 3rd rib. At the level of the 3rd and 4th ribs, you will be able to see three muscle layers: pectoral major, pectoralis minor, and serratus anterior muscles.

Figure 1. Superficial anatomy and probe position
For the PECS I block, after image optimization, the needle is inserted medial to lateral in an oblique manner until the tip enters the plane between the pectoralis major and minor muscles between the 3rd and 4th ribs, and 10 ml of local anesthetic is injected under ultrasound guidance while visualizing the spread of local anesthetic in the plane between the muscle layers.
For the PECS II block, the needle is then advanced into the plane between the pectoralis minor and serratus muscles, and 20 ml of local anesthetic is injected watching for spread between the muscle layers under ultrasound guidance.
Clinical Evidence
After the initial description by Blanco[1-3], there are only a few published trials on PECS blocks. A study by Wabha[6] in 2014 compared PECS I/II blocks to paravertebral blocks at T4 in patients undergoing modified radical mastectomy. The study found that the patients who received PECS blocks had lower intraoperative opioid consumption and better pain control postoperatively. Bashandi[7] randomized 120 patients to PECS I/II blocks plus general anesthesia versus general anesthesia alone and no blocks. Patients in the PECS I/II group had statistically significant lower VAS pain scores, lower intraoperative fentanyl use, lower total amount of morphine to keep VAS < 3, shorter PACU stay, lower PACU sedation scores, and shorter post-surgical hospital stays.
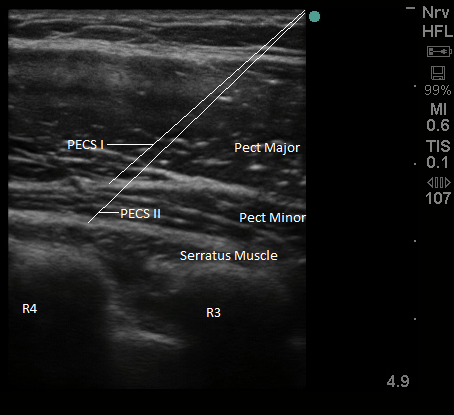
Figure 2. Sonoanatomy and needle tip placement for PECS I/II
Most recently, Kulhari[8] compared PECS II block to thoracic paravertebral blocks performed at T3 in 40 patients undergoing modified radical mastectomy. Both groups received blocks with 25 ml of ropivacaine 0.5% and had a morphine PCA for postoperative analgesia. Patients in the PECS group had decreased 24 morphine requirements, lower pain scores, and longer duration of analgesia.
Conclusion
PECS I/II blocks have become popular since first described. It is a relatively easy to learn technique which appears to be a good choice for analgesia in patients undergoing breast surgery. It is expected that more randomized trials will be published in the coming years, especially comparing the technique to paravertebral blocks.
References
- Blanco R. The ‘pecs block’: a novel technique for providing analgesia after breast surgery. Anaesthesia 2011; 66: 847-8.
- Blanco R, Fajardo M, Parras Maldonado T. Ultrasound description of pecs II (modified pecs I): a novel approach to breast surgery. Rev Esp de Anestesiol Reanim 2012; 59: 470–5.
- Blanco R, Parras T, McDonnell G, Prats-Galino A. Serratus plane block: a novel ultrasound-guided thoracic wall nerve block. Anaesthesia 2013; 68: 1107-13.
- Fujiwara A, Komasaw N, Minami T. Pectoral nerves (pecs) and intercostal nerve block for cardiac resynchronization therapy device implantation. Springerplus 2014; 3: 1049.
- Purcell N, Wu D. Novel use of the pecs II block for upper limb fistula surgery. Anaesthesia 2014; 69: 1294.
- Wahba SS, Kamal SM. Thoracic paravertebral block versus pectoral nerve block for analgesia after breast surgery. Egyptian J Anaesth 2014; 30: 129-35.
- Bashandi GM, Abbas DN. Pectoral nerves I and II blocks in multimodal analgesia for breast cancer surgery: a randomized clinical trial. Reg Anesth Pain Med 2015; 40: 68-74.
- Kulhari S, Bharti N, Bala I, Arora S, Singh G. Efficacy of pectoral nerve block versus thoracic paravertebral block for postoperative analgesia after radical mastectomy: a randomized controlled trial. Br J Anaesth 2016; 117:382-6.