How I Do It
Learn from your colleagues. ASRA Pain Medicine members share how they perform common procedures and accomplish other tasks.
- Listed by publication date, most recent on top
How I Do It: Genicular Nerve Blocks for Acute Pain
Cite as: Dunworth S, Gadsden J. How I do it: genicular nerve blocks for acute pain. ASRA Pain Medicine News 2022;47. https://doi.org/10.52211/asra050122.018
Introduction
Regional analgesia is a foundational component of multimodal postoperative pain management following knee replacement surgery (TKA). Targeted, motor-sparing regional techniques such as adductor canal blocks and posterior capsule infiltration (aka IPACK) provide good pain control while facilitating early ambulation and rehab.1,2 However, many patients continue to experience significant pain after TKA, even when these two blocks are performed. This is not surprising, as the anterior knee is innervated by the saphenous nerve, articular branches of the nerves to the three vastus muscles (medialis, intermedius, and lateralis), and at least four genicular nerves. Only two of these nerves (the saphenous and nerve to vastus medialis) are covered by a standard adductor canal block. Targeted genicular nerve blocks (or ablative procedures) have been a standard chronic pain intervention for arthritic pain in the past.3 Recently, it was shown that the addition of genicular nerve blockade for TKA patients can significantly reduce postoperative opioid requirement,4 and since these blocks are simple and quick to perform, they are an impactful addition to our block pathway for knee arthroplasty patients.
Anatomy
An overview of knee innervation is presented in Figure 1. The posterior knee is innervated largely by the popliteal plexus, derived from the tibial and obturator nerves. The anterior knee joint and capsule are supplied by four branches of the femoral nerve (the saphenous nerve and articular branches of the nerves to the three vasti), as well as multiple branches from the sciatic nerve. The cardinal genicular nerves are named for their position relative to the knee joint: the superomedial genicular nerve (SMGN), the superolateral genicular nerve (SLGN), and the inferomedial (IMGN) and inferolateral (ILGN) genicular nerves. These genicular nerves “wrap around” from behind to the anterior aspect of the knee, and their consistent proximity to the metaphysis of the femur and tibia make them easy targets for blockade. Some cadaveric sources describe the superomedial genicular nerve as originating from a branch of the femoral nerve; while interindividual variation exists, the upstream origin of this branch is not important from a clinical perspective, as its eventual location just proximal to the medial epicondyle is consistent.
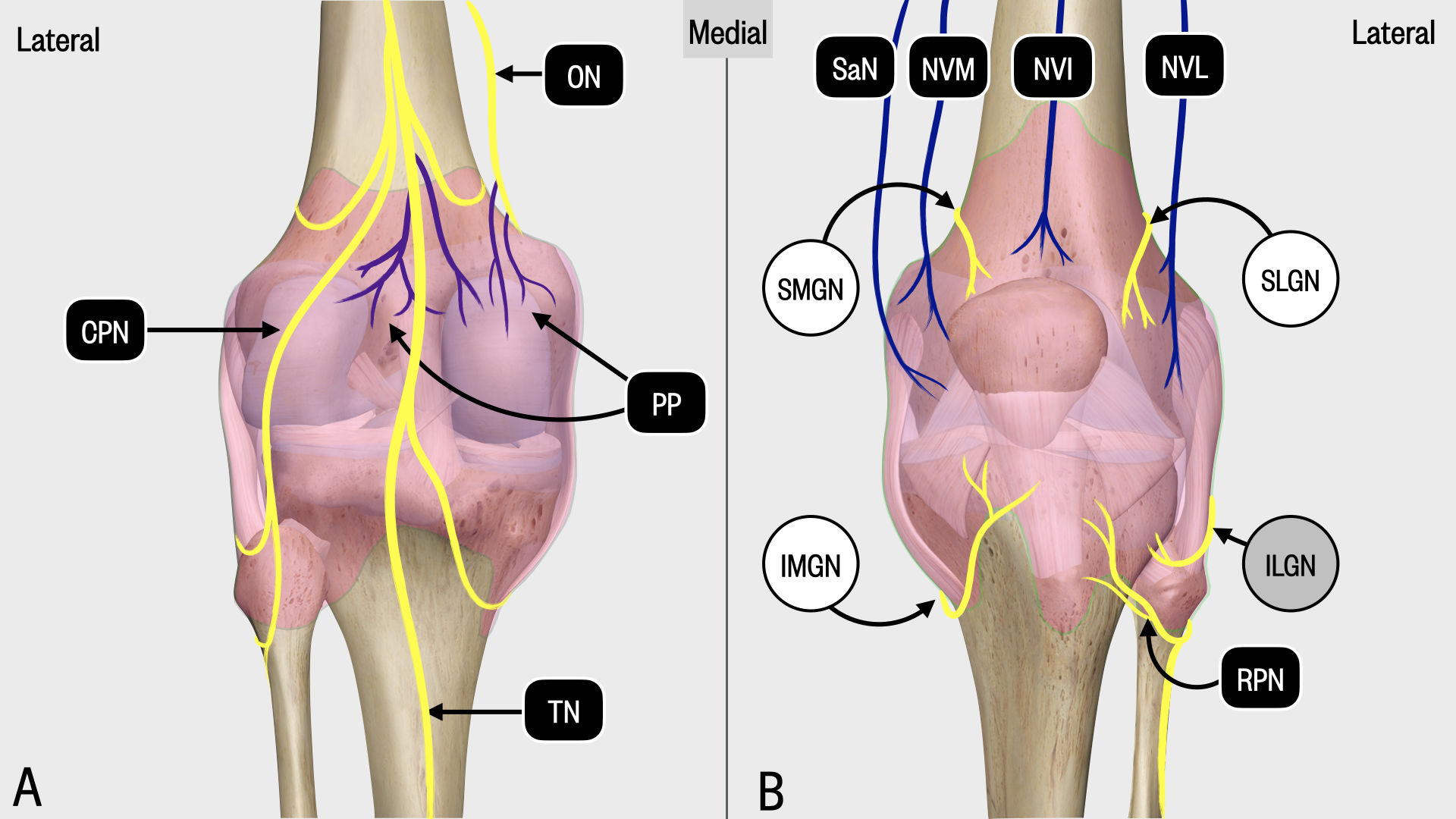
Figure 1. Schematic diagram showing posterior (A) and anterior (B) innervation of the knee capsule and joint. The three genicular targets are the SMGN, SLGN and IMGN. ILGN, inferolateral genicular nerve; IMGN, inferomedial genicular nerve; NVI, nerve to vastus intermedius; NVL, nerve to vastus lateralis; NVM, nerve to vastus medialis; RPN, recurrent peroneal nerve; SaN, saphenous nerve; SLGN, superolateral genicular nerve; SMGN, superomedial genicular nerve.
Sonoanatomy and Technique
Our genicular nerve block technique involves blockade of three of the genicular nerves (superolateral, superomedial, and inferomedial) as they travel around the femur and tibia toward the anterior capsule. We omit the inferolateral genicular nerve because it runs in close proximity to the common peroneal nerve, and blockade at this site may result in temporary foot drop. Finally, we also block the nerve to vastus intermedius, as it lies on the anterior surface of the femur just proximal to the patella, making it an easy additional target.
We perform genicular nerve blocks using a high-frequency linear transducer with patients in the supine position. For each of the three genicular nerves, the ultrasound transducer is placed on the lower limb in the sagittal orientation so that the bony cortex of either the femur (for the SMGN and SLGN) or the tibia (IMGN) is visualized (Figure 2). The position of the transducer is then adjusted, often by sliding toward the joint until a slight sloping of the epicondyle is seen near the metaphyseal-epiphyseal line. With proper probe placement for the SMGN and SLGN, the centerline of the probe will approximately align with the superior aspect of the patella. In this position, a small genicular artery often can be observed on the surface of the bone (although not always). For the IMGN, placement of the probe on the proximal tibia will reveal a shallow “bowl” through which the nerve courses. After the correct view is obtained and the skin is disinfected, we insert a 21G insulated block needle in an out-of-plane approach until contact is made with the bone. Following negative aspiration, 5 mL of local anesthetic is deposited. Under ultrasound visualization, the local anesthetic can be seen spreading along the bone and elevating the overlying soft tissue (Figure 3).
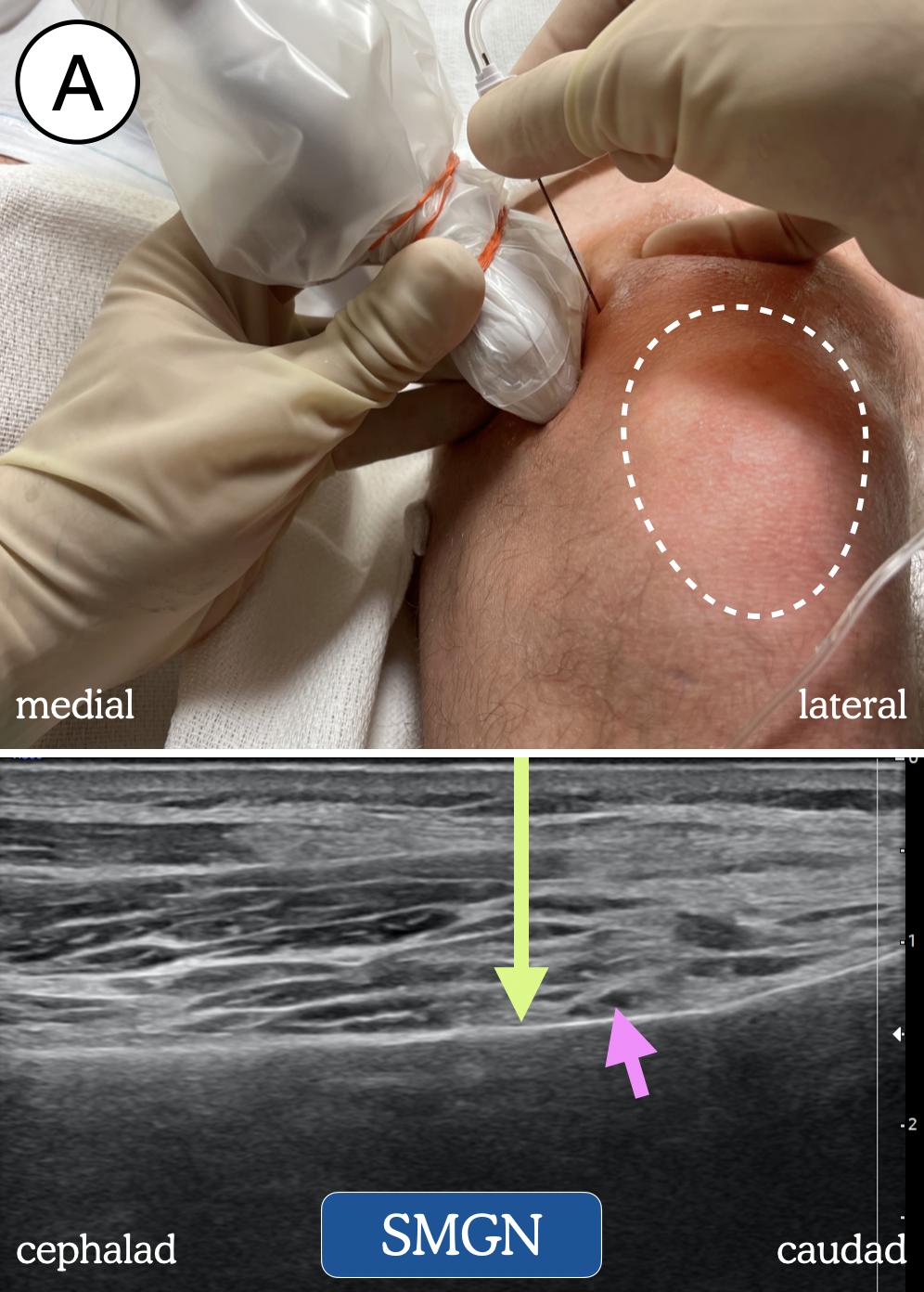 | 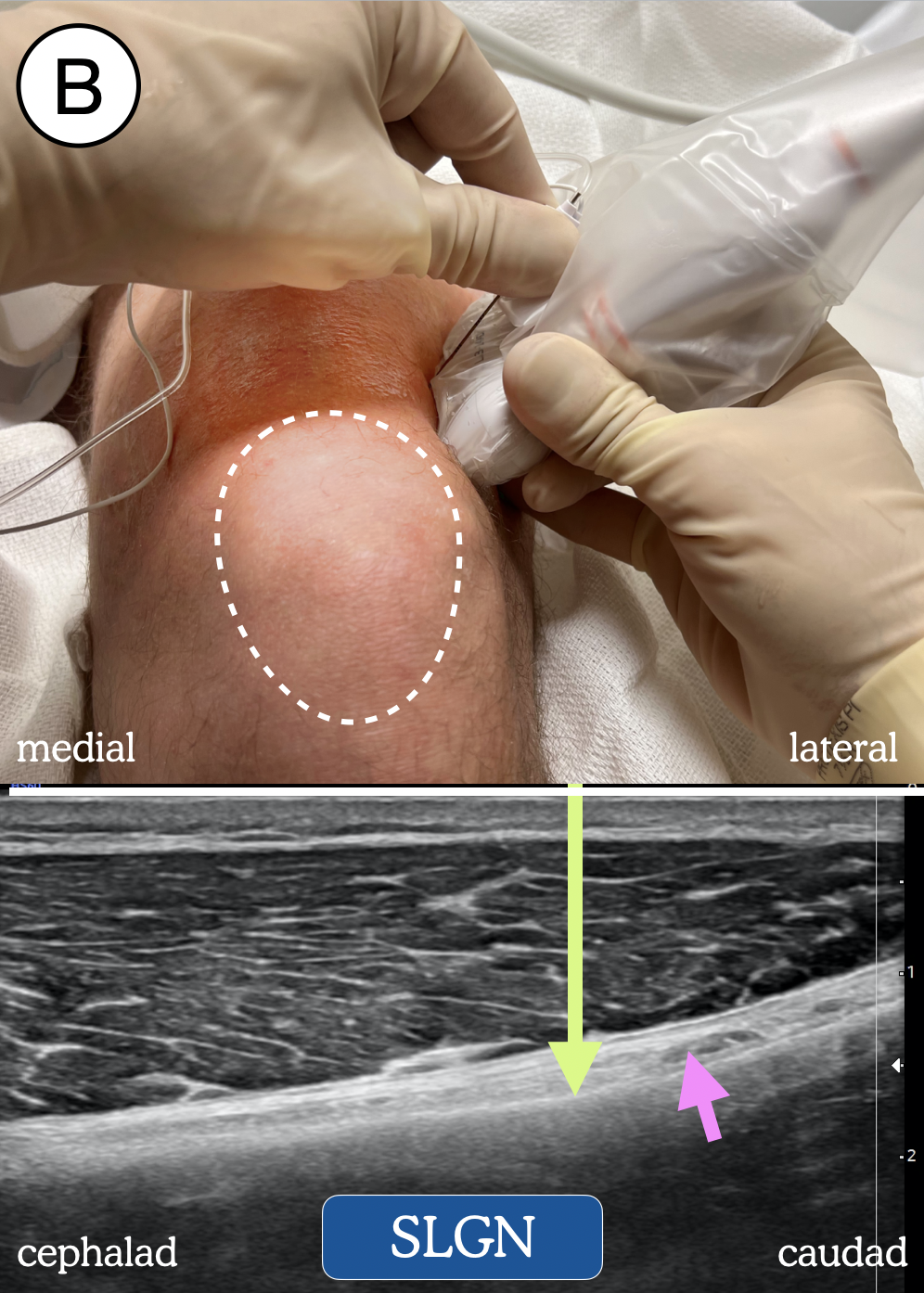 | 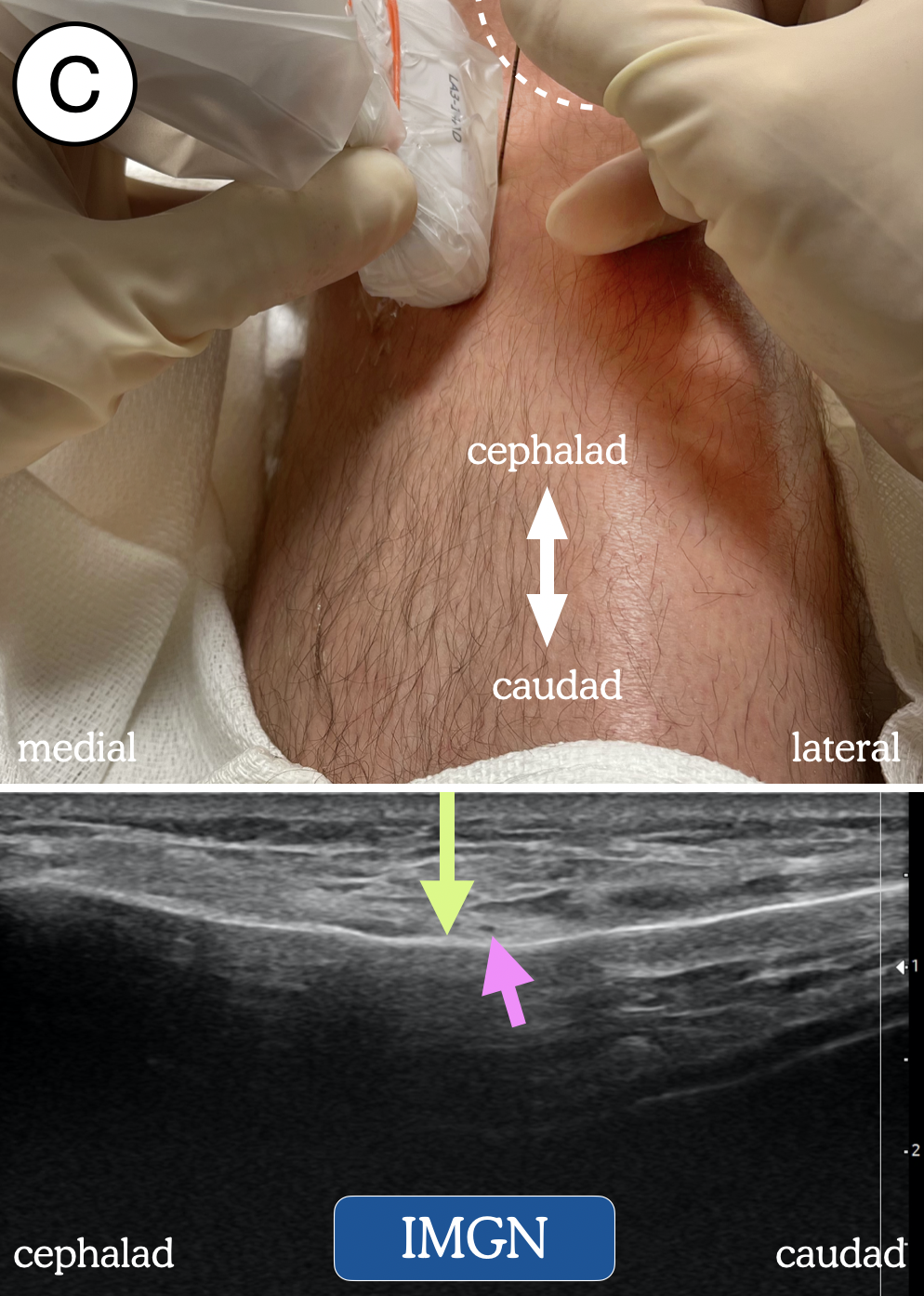 | 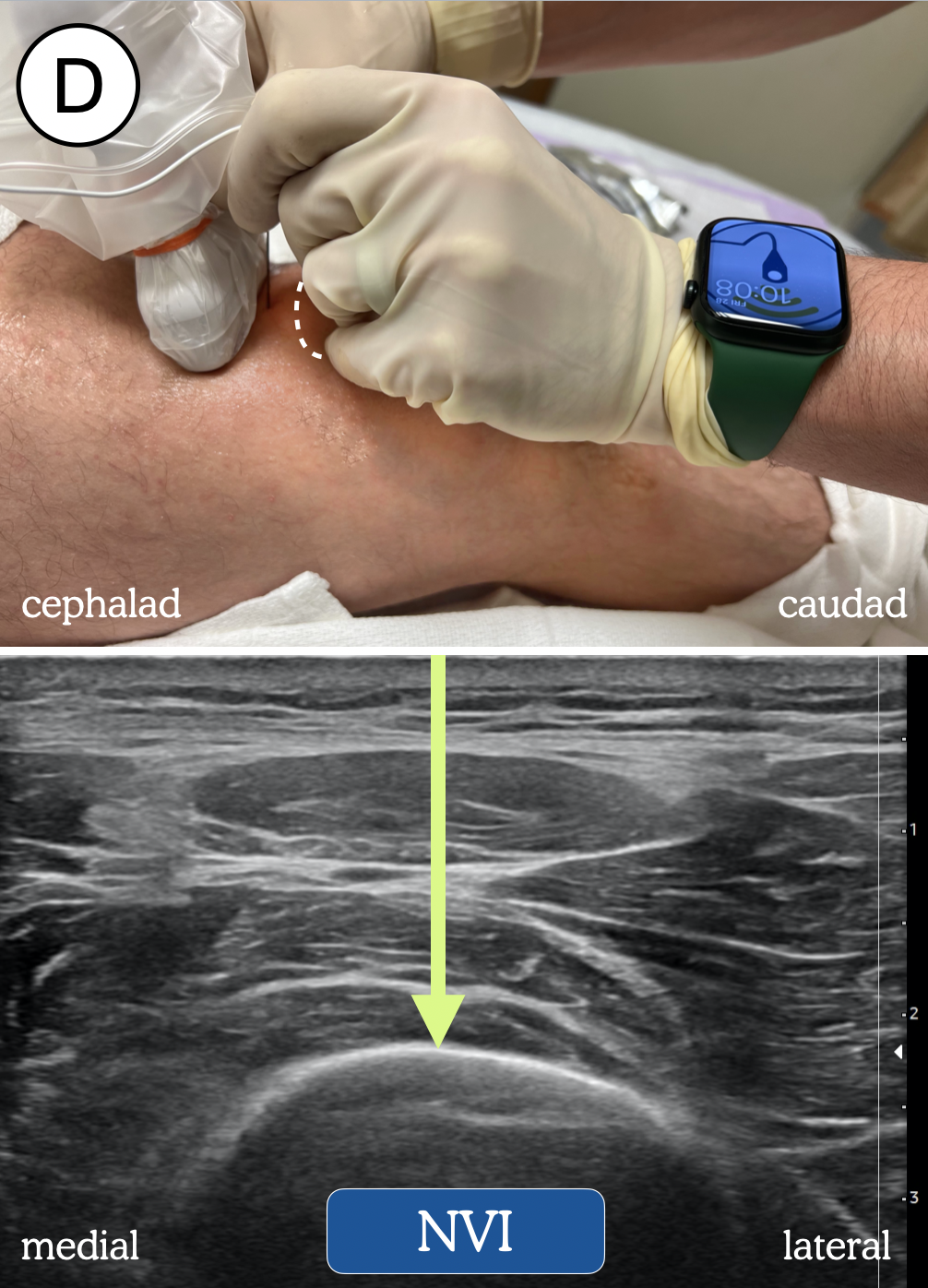 |
Figure 2. Transducer and needle position blockade of: (A) superomedial genicular nerve (SMGN); (B) superolateral genicular nerve (SLGN); (C) inferomedial genicular nerve (IMGN); and (D) the nerve to vastus intermedius (NVI). Dotted line represents outline of patella. Green arrow = needle trajectory and end-point. Pink arrow = genicular artery.
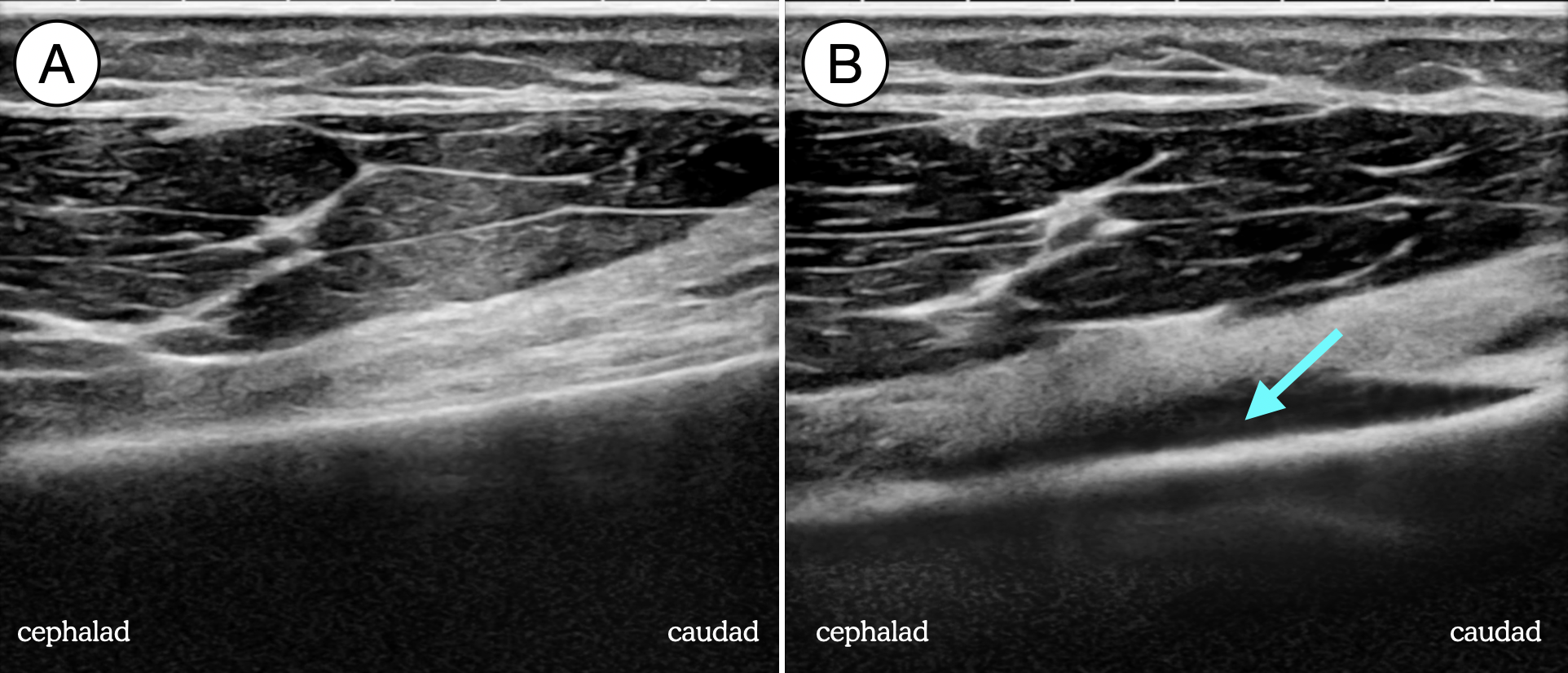
Figure 3. Superomedial genicular nerve block pre-injection (A) and post-injection (B), showing the spread of local anesthetic (blue arrow) along the cortex of the distal femur.
Nerve to the Vastus Intermedius
For the nerve to vastus intermedius, the transducer is placed about 3 cm superior to the patella in the transverse plane. The femur is visualized in short axis (Figure 2). Similar to the three genicular nerves, the needle is inserted in an out-of-plane approach until contact is made with the femur. Local anesthetic spread (5 mL) should be observed along the bone with elevation of the vastus intermedius muscle.
Choice of Local Anesthetic
We recommend using a long-acting local anesthetic to leverage the effect of the block for as long as possible. In our practice, we will typically prepare a 20 mL syringe of 0.25% bupivacaine with 1:400,000 epinephrine and 2 mg dexamethasone and use 5 mL of that mixture at each site.
Discussion
Genicular nerve blocks (including blockade of the SMGN, SLGN, IMGN and NVI) are an effective and efficient way to improve postoperative analgesia for patients undergoing TKA.4 Since the technique involves bony contact as the end-point for needle advancement (in contrast to a potentially difficult-to-visualize, nuanced fascial plane), these blocks are very easy to teach and learn. They also can be performed quickly — all four blocks take less than two minutes to perform in our practice.
Although not a complete answer on their own, genicular blocks address a “missing component” in traditional protocol of adductor canal and iPACK blocks, and we have observed earlier ambulation, improved pain control, and better overall recovery in this population since they have been implemented.
Clinical Pearls
- With our genicular nerve block set, we actually block four nerves: the nerve to the vastus intermedius and the superomedial, superolateral, and inferomedial genicular nerves.
- These blocks are generally well-tolerated in the awake patient with some sedation. That said, our practice is to perform a spinal anesthetic first in the preop block area, followed by the three peripheral blocks (adductor canal, iPACK, geniculars) to provide maximum comfort.
- These blocks can be performed with either an in-plane or out-of-plane technique. An in-plane technique requires alignment of three objects—the ultrasound beam, long axis of the bone, and the needle, and this can be challenging, especially in large patients. The out-of-plane technique (which we recommend) only requires alignment of the beam and bone, then a perpendicular insertion of the needle until bony contact is made.
- The genicular artery often is seen (especially if the Doppler function is employed) on the surface of the bone and should be thought of as a reassuring landmark that the corresponding nerve is nearby. However, the artery is not always seen, and the best sonographic target for local anesthetic deposition is the “bottom of the slope” where the femoral diaphysis meets metaphysis (SMGN, SLGN) or the “bowl” of the tibia (IMGN).
- If bupivacaine is used for the spinal anesthetic (eg, 0.5% isobaric bupivacaine), the leftover local anesthetic from the vial can be used (neat or diluted) for cost efficiency.

Sophia Dunworth, MD, is a regional anesthesiology and acute pain medicine fellow at Duke University School of Medicine in Durham, NC.
Jeff Gadsden, MD, FRCPC, FANZCA, is an associate professor of anesthesiology at Duke University School of Medicine in Durham, NC.
References
- Hanson NA, Allen CJ, Hostetter LS, et al. Continuous ultrasound-guided adductor canal block for total knee arthroplasty. Anesth Analg 2014;118(6):1370-7. https://doi.org/10.1097/MD.0000000000020320
- Ochroch J, Qi V, Badiola I, et al. Analgesic efficacy of adding the IPACK block to a multimodal analgesia protocol for primary total knee arthroplasty. Reg Anesth Pain Med 2020;45(10):799-804. http://dx.doi.org/10.1136/rapm-2020-101558
- Vanneste B, Tomlinson J, Desmet M, Krol A. Feasibility of an ultrasound-guided approach to radiofrequency ablation of the superolateral, superomedial and inferomedial genicular nerves: a cadaveric study. Reg Anesth Pain Med 2019;44(10):966, http://dx.doi.org/10.1136/rapm-2019-100381
- Rambhia M, Chen A, Kumar AH, et al. Ultrasound-guided genicular nerve blocks following total knee arthroplasty: a randomized, double-blind, placebo-controlled trial. Reg Anesth Pain Med 2021;46:862-6. http://dx.doi.org/10.1136/rapm-2021-102667
Leave a commentOrder by
Newest on top Oldest on top