How I Do It: Gasserian Ganglion Block for Trigeminal Neuralgia
Cite as: Chaturvedi A, Dorado F, Shanthanna H, et al. How I do it: gasserian ganglion block for trigeminal neuralgia. ASRA Pain Medicine News 2023;48. https://doi.org/10.52211/asra050123.011.
The latest (2018) International Classification of Headache Disorders-3 (ICHD3) lays out three etiological categories of trigeminal neuralgia (TN): classical TN (neurovascular compression), secondary TN (due to other causes), and idiopathic TN (no neurovascular compression). TN is characterized by recurrent short episodes of sharp, electrical shock like pain, typically abrupt in onset and termination, along the distribution of one or more divisions of the trigeminal nerve. These episodes can be triggered by trivial stimuli or be spontaneous in nature. Treatment modalities include pharmacotherapy, rhizotomy, and microvascular decompression. No randomized clinical trial aiming to directly compare these interventions has been published to date.
Microvascular decompression (MVD) offers long-term relief in classical TN for approximately 62% - 89% of patients.1 However, ablative procedures like radiofrequency ablation and glycerol neurolysis have also shown similar efficacy in this patient population (26%-82%, and 19%-58% respectively).1 In idiopathic TN, chemical neurolysis with glycerol, radiofrequency ablation, or balloon rhizotomy of the gasserian ganglion are the preferred treatment choices over MVD. These radiofrequency ablative procedures may also be beneficial for patients who failed or are not candidates for MVD.2
Secondary TNs may also be an indication for neuroablative therapies of the gasserian ganglion. In addition, trigeminal ganglion interventions have also been used to palliate cancer pain involving cranial or base of the skull structures. Similarly, they have also been found to have a role in the treatment of chronic intractable cluster headaches3,4 and persistent idiopathic facial pain.5
The reported complications to these approaches are variable. Radiofrequency thermocoagulation (RFTC) is associated with the highest incidence of facial and corneal hypoesthesia (1%–20.3%)6 and trigeminal motor weakness (3%–29%).6 The incidence of anesthesia dolorosa is around 0.5%–1%.1
The trigeminal nerve supplies the sensory innervation to the face as well as the sensory and motor innervation to the mastication muscles. The nerve has three major divisions:
- Ophthalmic V1
- Maxillary V2
- Mandibular V3
The nerve originates from the midlateral surface of pons. Its sensory ganglion (the gasserian ganglion) resides in Meckel’s cave, which is in the floor of the middle cranial fossa. There are several important structures that reside in the vicinity of the ganglion: the cavernous sinus, the optic and trochlear nerves medially, the inferior surface of the temporal lobe of the brain superiorly, and the brain stem posteriorly.7 Furthermore, the ganglion has a somatotropic distribution: thus the mandibular portion lies in the rostral and lateral part, the maxillary division does in the middle portion, and the ophthalmic division does in the cephalad and medial region.5 The ophthalmic division leaves the ganglion to reach the orbit through the superior orbital fissure. It divides into the supraorbital, supratrochlear, and nasociliary nerves to supply the forehead and nose. The maxillary division exits the middle cranial fossa from foramen rotundum and enters the orbit through the inferior orbital fissure. The mandibular division exits through the foramen ovale (FO) and divides into the buccal, lingual, inferior alveolar, and auriculotemporal nerves.
Meckel’s cave can be percutaneously accessed to perform ablative interventions, which are regularly preceded by a positive diagnostic block. The needling process is described below, which is the same regardless of the planned intervention, but with different equipment.
Procedure
Formal consent explaining the risks, benefits, and alternative options should be obtained from the patient. A peripheral IV is placed prior to the procedure for sedation and resuscitation if needed. Basic monitoring must be instituted as in any major nerve block. Electrocardiogram, non-invasive blood pressure, and pulsoximetry are sufficient for timely identification of acute hemodynamic changes due to sedation and/or autonomic reflexes elicited during the procedure. Awareness of absolute contraindications should be granted. Those include local infection, sepsis, coagulopathy, increased intracranial pressure, allergy to local anesthetics, and refusing to collaborate.
A formal time-out is performed immediately prior to the procedure, confirming correct patient, site, and procedure. The patient is placed supine on the table with a shoulder roll to assist with maximal head extension as tolerated, thereby facilitating an optimal submental view with fluoroscopy (Figure 1). The correct side of the face is marked. Using sterile technique, the skin overlying the procedural region is prepped with betadine solution and draped leaving the eye exposed.
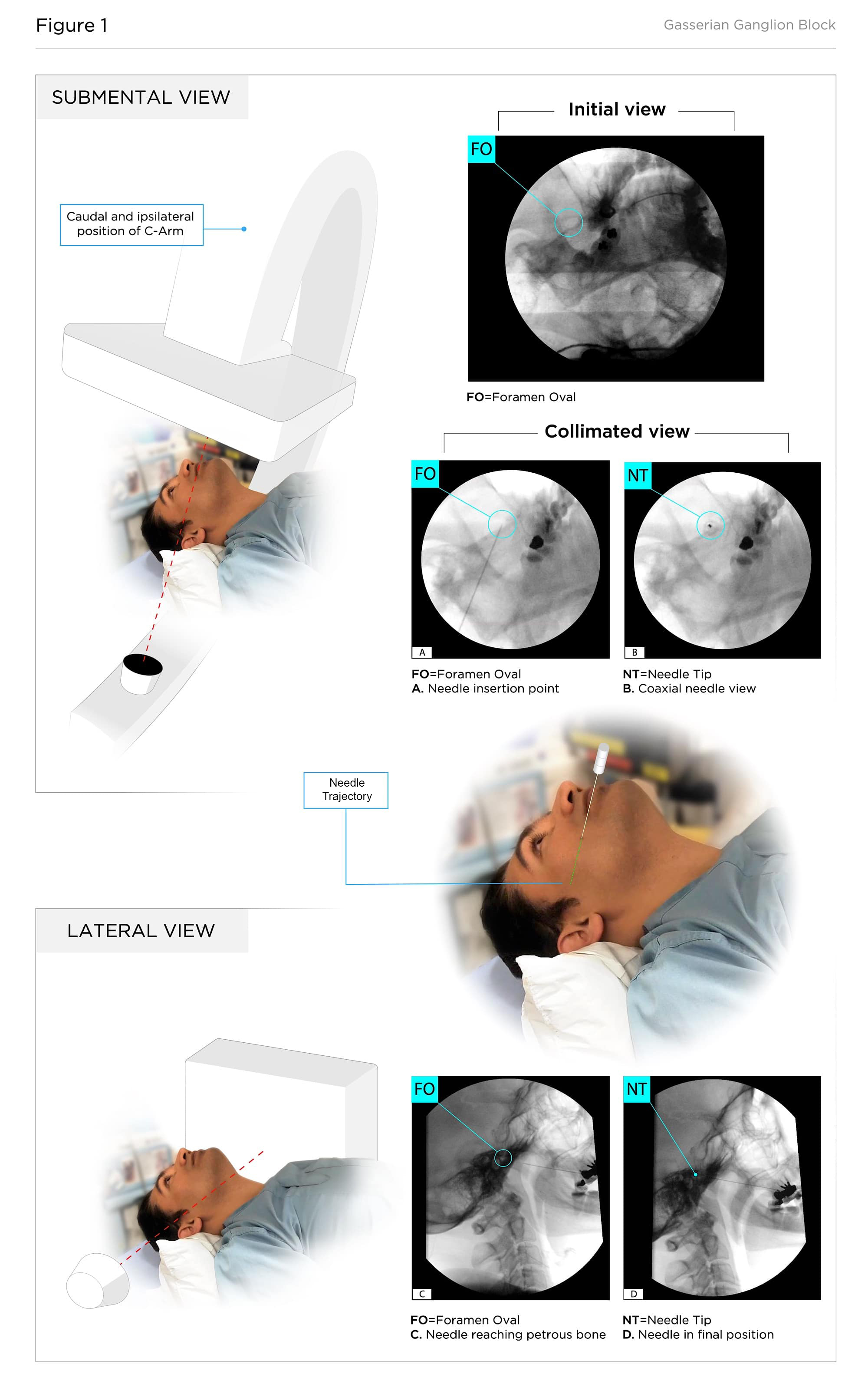
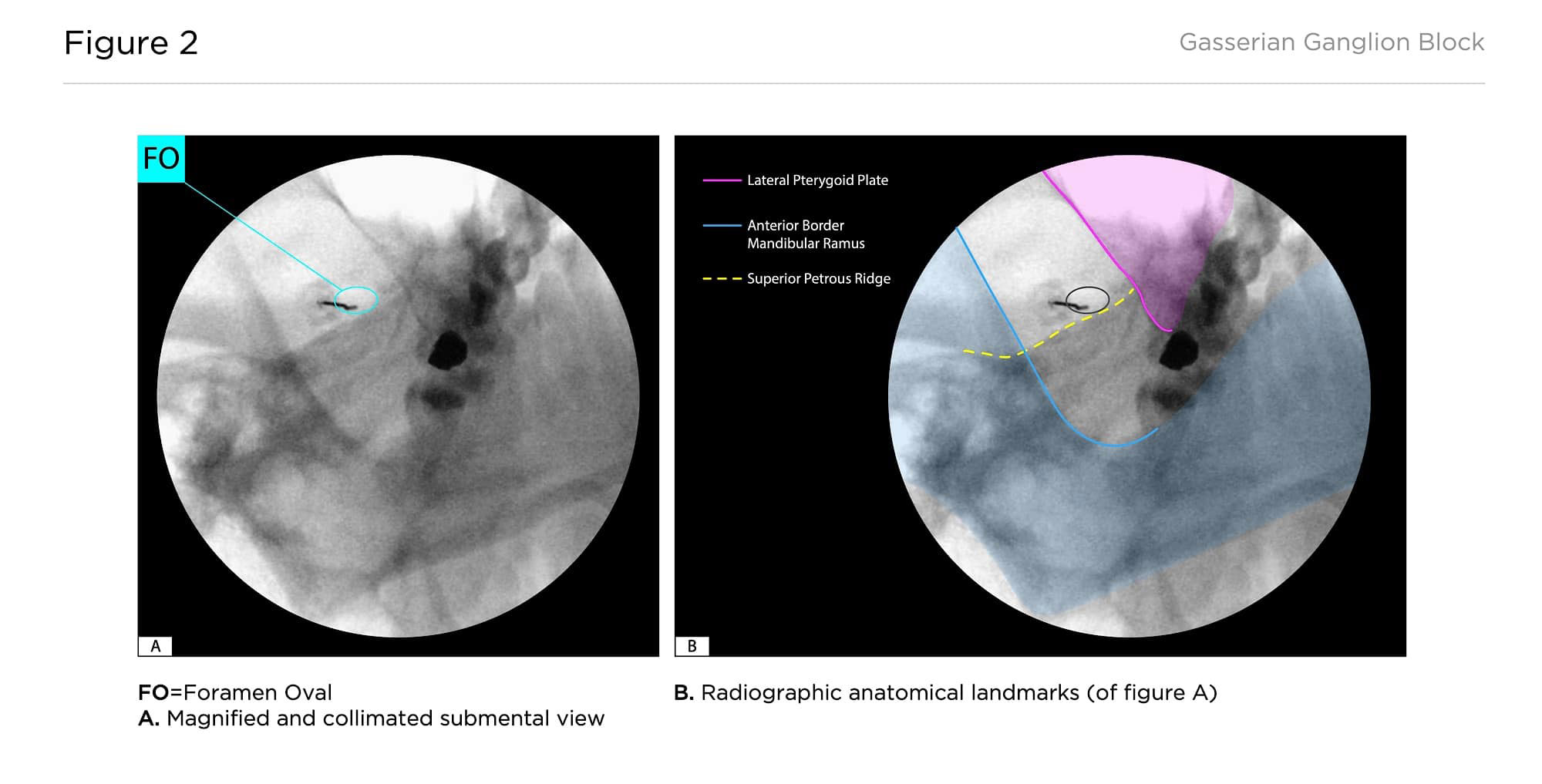
Utilizing intermittent fluoroscopy, the FO is localized. The C-arm image intensifier should tilt caudally 15-20 degrees and oblique ipsilaterally 5-10 degrees to bring the FO into view just at the inferior aspect of the space between the coronoid apophysis of the mandible, and the superior petrous ridge.8 The image must be magnified and collimated to focus on the FO (Figure 2).9,10,11
The skin and subcutaneous tissues are anesthetized with 2 mL of 1% lidocaine using a 27G needle raising the skin wheal directly over the shadow of the foramen, which is approximately 2-2.5 cm lateral and 1 cm inferior to the ipsilateral angle of mouth. A 10 cm 25G Quincke needle with its tip bent to help steering is inserted and advanced with intermittent fluoroscopic guidance in a co-axial view until reaching the foramen.
As the needle enters the FO, the patient may experience discomfort within the mandibular distribution indicating needle proximity to the V3 nerve root, and the patient should be reassured.
Attention should be given to the trigemino-cardiac reflex (TCR) upon the needle entering the FO. TCR is defined as the sudden onset of parasympathetic dysrhythmia including profound bradycardia, sympathetic hypotension, apnea, or gastric hypermotility. Thus, atropine or glycopyrrolate should be readily available. If the TCR is encountered, the needle should be withdrawn immediately, and the anesthetic care provider should be prepared to administer any of those medications intravenously. Pre-emptive administration could be advisable in certain cases.
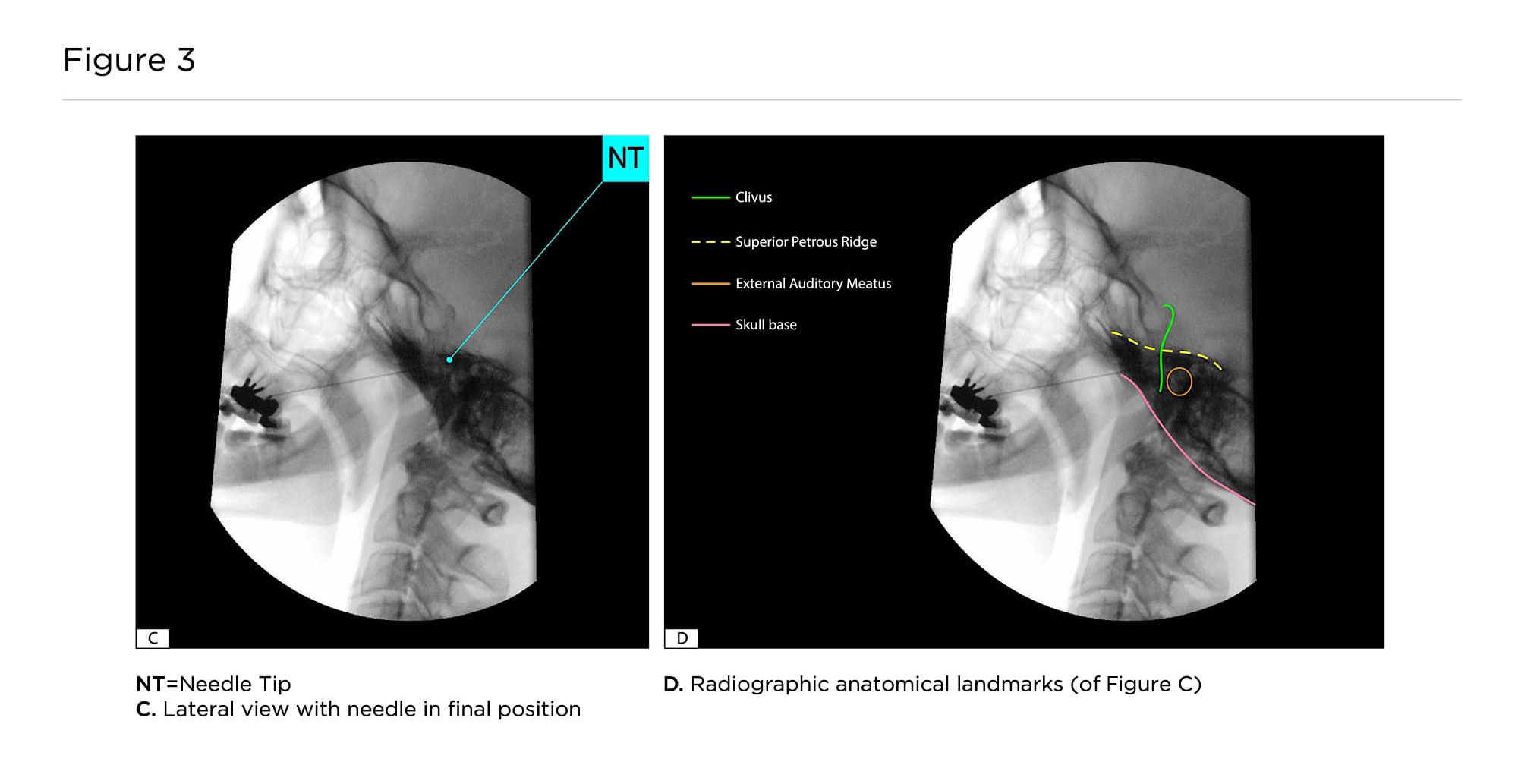
Subsequently, lateral fluoroscopic imaging is used to obtain a sagittal image of the clivus bone (Figure 3). The fluoroscope is wig-wagged to ensure minimization of parallax error. The auditory meatuses are lined up. The needle tip is advanced through the foramen in the lateral view under fluoroscopic guidance, with slight resistance as it penetrates the pterygoalar ligament. Precaution is taken not to advance the tip past the shadow of the clivus, remaining anterior to the petrous bone at all times.
The stylet is removed to check for any cerebrospinal fluid (CSF) or blood. Ensuring no CSF or blood is aspirated, medication is subsequently injected in 0.25mL aliquots. Long-acting local anesthetics are used for diagnostic blocks. Titrated injection in small aliquots (<0.25mL of local anesthetic) and continuous communication with the patient allows for early detection of brainstem injection. Risk of total brainstem anesthesia can also be reduced by careful aspiration of the needle prior to injection. Finally, the needle is flushed and withdrawn.
After successful diagnostic blockade of the gasserian ganglion, RFTC, glycerol neurolysis, or balloon rhizotomy can be planned for long-term relief. Specific ablative procedures may require different medications and/or solutions, but the needle placement is similar to the diagnostic block.
Discussion
Pain due to TN can be quite debilitating and disturbing for patients, affecting their day-to-day life. Percutaneous gasserian ganglion interventions are available options that have been proven to be successful in providing long-lasting pain relief.6 These techniques may be considered in lieu of surgical alternatives, such as microvascular decompression. Although these procedures are of high complexity, life threatening complications are rare.12
Percutaneous gasserian ganglion interventions are available options that have been proven to be successful in providing long-lasting pain relief.
Injury to intracranial vascular and neural structures are more likely with misplacement of the needle tip outside of safety margins.11,13,14 To avoid the internal carotid artery into the cavernous sinuous, which could lead to a carotid cavernous fistula, oblique tilt of the C-arm should be kept at the minimum required for an adequate view of the FO. Directing the needle in a more pronounced medial direction can increase the possibility of vessel puncture. Furthermore, risk of injury to neural structures (eg, cranial nerves IV, VI, VIII, brainstem) can be reduced by keeping the tip of the needle within a safe distance of the clivus border in the lateral view (2-4mm). Hence, appropriate alignment of the auditory meatuses in the lateral view is extremely important for safe execution of this procedure.
Appropriate depth of sedation and continuous communication with the patient contribute to lessening the burden of the procedure and comfort the patient. Neurological assessment should be done continuously during the final positioning of the needle in the FO and also during injection. Neurologic symptoms, such as seizures, loss of consciousness, and apnea, could be caused by intravascular or intrathecal injection of local anesthetic.
Clinical Pearls
- Patient cooperation and sedation is the key for a satisfactory procedure.
- Risks specific to the gasserian ganglion block like retrobulbar hematoma, cheek hematoma, keratitis due to loss of corneal reflex, meningitis, transient bradycardia, anesthesia dolorosa, and mandibular spasm should be well described to the patient.
- The most important aspect of this block is to obtain a fluoroscopic coaxial view of the needle approaching the FO and a lateral view to control the depth of the needle tip position.
- The needle tip should always be curved to help with steering and positioning.
- Needle manipulation at the border of the FO can be very painful for the patient, but it is an important clue to correct needle placement.
- If CSF drainage is encountered during the procedure, the needle should be withdrawn until no fluid is appreciated. If CSF continues to be aspirated even after adjustment of the needle tip, abandonment of the procedure is advisable.4,10
- Subarachnoid and/or intravascular injection, which may cause total spinal anesthesia or signs of neurotoxicity, should be monitored closely. Slow injection and small aliquots of the chosen solution allow for early detection of those complications.

Apoorv Chaturvedi MBBS, DNB, is a chronic pain fellow in the Department of Anesthesia and Pain Medicine at St. Michael’s Hospital at the University of Toronto in Canada.

Fabian camilo Dorado velasco, MD, is a chronic pain fellow in the Department of Anesthesia and Pain Medicine at St. Michael’s Hospital at the University of Toronto in Canada.

Harsha Shanthanna, MD, PhD, FRCPC, is an associate professor in the department of Anesthesia at McMaster University in Hamilton, Canada.
Xiang Qian, MD, PhD, is a clinical professor of anesthesiology, perioperative, and pain Medicine at Stanford University in California.

Akash Goel, MD, MPH, FRCPC, is an assistant professor in the department of Anesthesia and Pain Medicine at the University of Toronto in Canada.
Note: Apoorv Chaturvedi and Fabian Dorado were equal contributors to this manuscript.
References
- Bendtsen L, Zakrzewska JM, Abbott J, et al. European Academy of Neurology guideline on trigeminal neuralgia. Eur J Neurol 2019;26(6):831-49. https://doi.org/10.1111/ene.13950
- Bendtsen L, Zakrzewska JM, Heinskou TB, et al. Advances in diagnosis, classification, pathophysiology, and management of trigeminal neuralgia. Lancet Neurol 2020;19(9):784-96. https://doi.org/10.1016/S1474-4422(20)30233-7
- Ekbom K, Lindgren L, Nilsson BY, et al. Retro-Gasserian glycerol injection in the treatment of chronic cluster headache. Cephalalgia 1987;7(1):21-7. https://doi.org/10.1046/j.1468-2982.1987.0701021.x
- Hassenbusch SJ, Kunkel RS, Kosmorsky GS, et al. Trigeminal cisternal injection of glycerol for treatment of chronic intractable cluster headaches. Neurosurgery 1991;29(4):504-8. https://doi.org/10.1097/00006123-199110000-00003
- Day M, Justiz R, Nader A. Head and neck blocks. In: Benzon H, Raja SN, Fishman S, et al. Essentials of Pain Medicine. 4th ed. New York, NY: Elsevier; 2018.
- Wang JY, Bender MT, Bettegowda C. Percutaneous procedures for the treatment of trigeminal neuralgia. Neurosurg Clin N Am 2016;27(3):277-95. https://doi.org/10.1016/j.nec.2016.02.005
- Di Muzio B, Shadwell J, Engelbrecht Z, et al. Meckel’s cave. Radiopaedia org 2022. https://doi.org/10.53347/rID-13218
- Rose KR, Stone JJ, Ren, Z, et al. Percutaneous trigeminal rhizotomy in a biplane angiosuite: technical assessment. J Neurointerv Surg 2014;6(9):699-703. http://dx.doi.org/10.1136/neurintsurg-2013-010883
- Benzon H, Raja SN, Fishman SE, et al. Essentials of Pain Medicine. Elsevier Health Sciences; 2011.
- Diwan S, Staats P. Atlas of Pain Medicine Procedures. New York, NY: McGraw Hill Professional; 2014.
- Peris-Celda M, Graziano F, Russo V, et al. Foramen ovale puncture, lesioning accuracy, and avoiding complications: microsurgical anatomy study with clinical implications. J Neurosurg 2013;119(5):1176-93. https://doi.org/10.3171/2013.1.JNS12743
- Zheng S, Yuan R, Ni J, et al. Long‐term recurrence‐free survival and complications of percutaneous balloon compression and radiofrequency thermocoagulation of Gasserian ganglion for trigeminal neuralgia: a retrospective study of 1313 cases. Pain Pract 2022;22(5):532-40. https://doi.org/10.1111/papr.13114
- Revilla-Pacheco F, Antón-Alonso A, Rodríguez-Salgado P, et al. Association between the symptomatic appearance of dural arteriovenous fistula and trigeminal ganglion radiofrequency thermocoagulation. NMC Case Rep J 2020;7(3):129-34. https://doi.org/10.2176/nmccrj.cr.2019-0197
- Smulders PS, Terheggen MA, Geurts JW, et al. Percutaneous radiofrequency treatment of the gasserian ganglion for trigeminal neuralgia complicated by trochlear nerve palsy: a case report. Reg Anesth Pain Med 2021;46(11):1002-5. https://doi.org/10.1136/rapm-2020-102285