POCUS Spotlight: Gastric Ultrasound
Cite as: Perlas A, Kruisselbrink R. POCUS spotlight: gastric ultrasound. ASRA News 2021;46. https://doi.org/10.52211/asra110121.065
Gastric point-of-care ultrasound (POCUS) is an accurate and reliable tool to objectively assess gastric content and aspiration risk at the bedside.1–3 It has been studied and applied in the adult,1,4,5 pediatric,6–8 obstetric,9–12 severely obese13,14 and emergency surgical populations.15 It is being adopted increasingly in anesthesia practice throughout the world.
The I-AIM (Indication, Acquisition, Interpretation and Medical Decision-Making) framework is a succinct and intuitive model for all POCUS examinations,16 and we recommend its use as a standardized approach to gastric POCUS to minimize error.17–19
Indication
Inaccurate aspiration risk assessment is an important cause of many pulmonary aspiration events, a highly morbid occurrence and the leading cause of death from anesthesia airway events.20–23 Thus, gastric POCUS is primarily indicated when gastric content is uncertain based on clinical information alone (ie, the pretest probability of a full or empty stomach is around 50%), such as with an unconfirmed fasting history (eg, pediatrics, language barrier, altered mental status), comorbid systemic disease affecting gastric emptying (eg, diabetic gastroparesis, end-stage renal or liver disease, neuromuscular disease), or emergency situations where delayed gastric emptying is common despite otherwise appropriate fasting intervals. In situations of equivocal aspiration risk, gastric ultrasound enables clinicians to objectively determine gastric contents, facilitating accurate and reliable risk stratification to guide clinical management.3,24,25
Acquisition
The gastric antrum is of greatest interest because of its consistent location and the available sonographic windows for all types of gastric content.1,4,25,26 The patient is scanned in the supine and then right lateral decubitus (RLD) positions. The RLD position is necessary for an accurate exam because it ensures that all gastric contents, particularly in low-volume states, have shifted toward the gravitationally dependent antrum and are accounted for in the scan.1,4
In adults, a curved array, low-frequency (2–5 MHz) transducer with abdominal settings is placed in the sagittal plane in the epigastric area. Moving the transducer in a slow, controlled pattern in the left-right and cephalad-caudad directions avoids oblique views, which can overestimate the amount of gastric content. The antrum is found superficially posterior to the rectus muscle, immediately adjacent to the left lobe of the liver and anterior to the pancreas and great vessels (Figure 1). The thoracic spine may be seen posterior to the great vessels, particularly in slim subjects or children (Figure 1). Critical identifying features of the stomach, which can help differentiate it from other hollow viscus, are a multilayered wall (though not all five layers are typically visualized with a curvilinear probe) and the consistent location adjacent to the liver edge with the great vessels, preferably the aorta, in the far field of the image.
Because peristalsis can dramatically change the antral size from second to second, it is important to view the antrum for at least 10–15 seconds to obtain a representative observation. This is particularly critical if a volume assessment is being performed because the antrum needs to be evaluated at rest, between peristaltic contractions for an accurate assessment.
Interpretation
A qualitative exam, and quantitative (or volume assessment) in some selected cases, is required to interpret a gastric POCUS. The extremes of content (empty or solid) are of obvious clinical significance.26 If no content is visible in the antrum in both the supine and right lateral decubitus positions, known as grade 0 antrum, we can be certain that the stomach is empty and the volume of the content approaches nil (Figure 1).1,5,18,19 Approximately 45%–50% of all fasting subjects with low aspiration risk have a grade 0 antrum.5,6,10,13,27
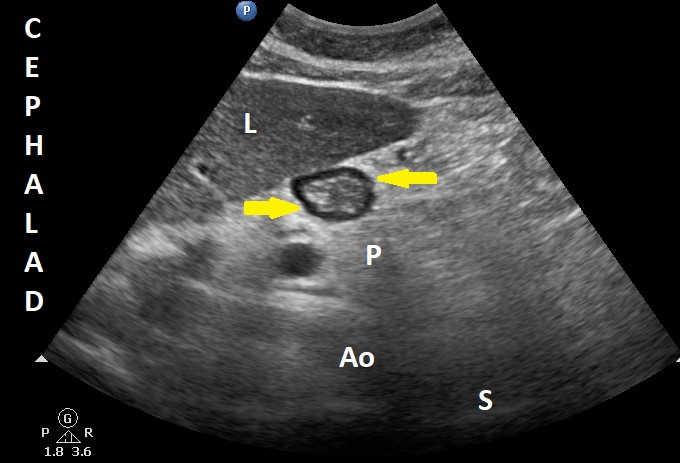
Figure 1. Sonographic image of the antrum in an empty stomach
The antrum appears empty in the right lateral decubitus position (grade 0 antrum).
Ao = aorta, L = liver, P = pancreas, and S = spine. Yellow arrows signal the antrum.
Used with permission from the Dr. Perlas Fontana Medicine Professional Corporation.
At the other end of the spectrum, thick fluid (hyperechoic) or solid content (heterogenous, mixed areas of high and low echogenicity, typically with an air component) in the antrum in any scanning position are unequivocal signs of a “full stomach” (Figure 2).26 A volume assessment is not required or recommended here, because any amount of thick fluid or solid is inconsistent with an “empty stomach.”18,19 Given that pulmonary aspiration of particulate content carries a dire prognosis, any amount of solid content in the stomach should be considered a full stomach and the patient should be managed accordingly.
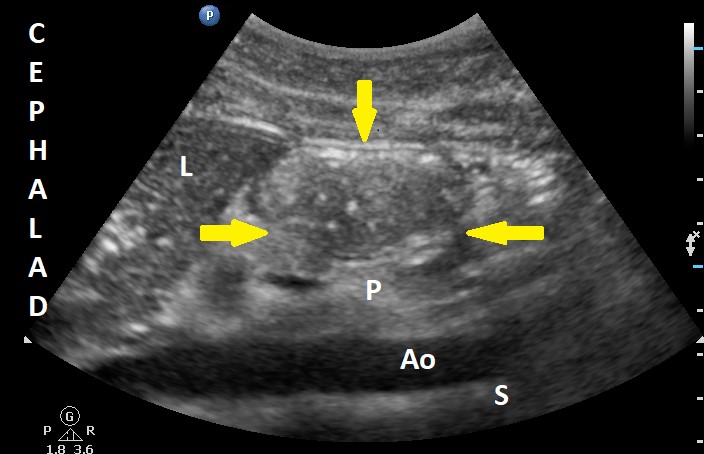
Figure 2. Sonographic image of the antrum with solid (hyperechoic) content
Ao = aorta, L = liver, P = pancreas, and S = spine. Yellow arrows signal the antrum.
Used with permission from the Dr. Perlas Fontana Medicine Professional Corporation.
On the other hand, when the antrum contains clear fluid (hypo or anechoic content; Figure 3), a volume assessment can help differentiate a low volume consistent with baseline gastric secretions versus a higher volume that could pose a risk for aspiration.1,4 A small volume of clear fluid (< 1.5 mL/kg), usually only evident in the right lateral decubitus position, known as grade 1 antrum, is a normal finding in about 45%–50% of fasting surgical patients.5,10,13 Conversely, a larger volume (> 1.5 mL/kg) often results in a distended antrum with clear fluid that is evident in both the supine and right lateral decubitus positions, known as grade 2 antrum. This is not a common finding in fasting surgical patients and suggests a volume in excess of baseline gastric secretions.5,10,13
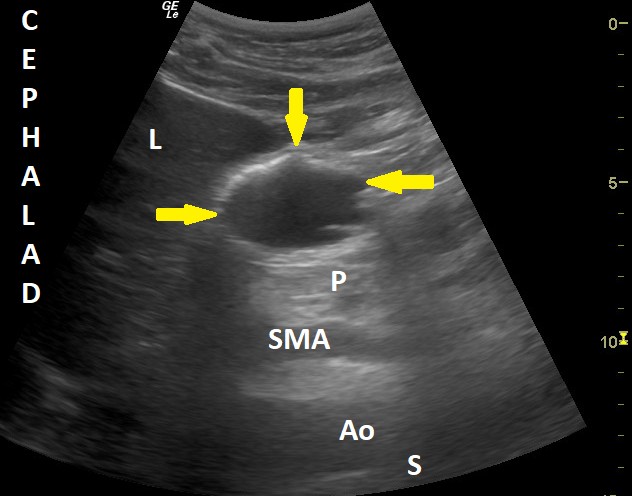
Figure 3. Sonographic image of the antrum with clear (hypoechoic) fluid content
Ao = aorta, L = liver, P = pancreas, S = spine, and SMA = superior mesenteric artery. Yellow arrows signal the empty antrum.
Used with permission from the Dr. Perlas Fontana Medicine Professional Corporation.
In the presence of clear fluids, a cross-sectional area of the gastric antrum, measured in a standardized manner at the level of the aorta in the right lateral decubitus, correlates with total gastric volume (Figure 4). This model is accurate and reliable for nonpregnant adults, with a wide-range of body mass indexes.1,2,14
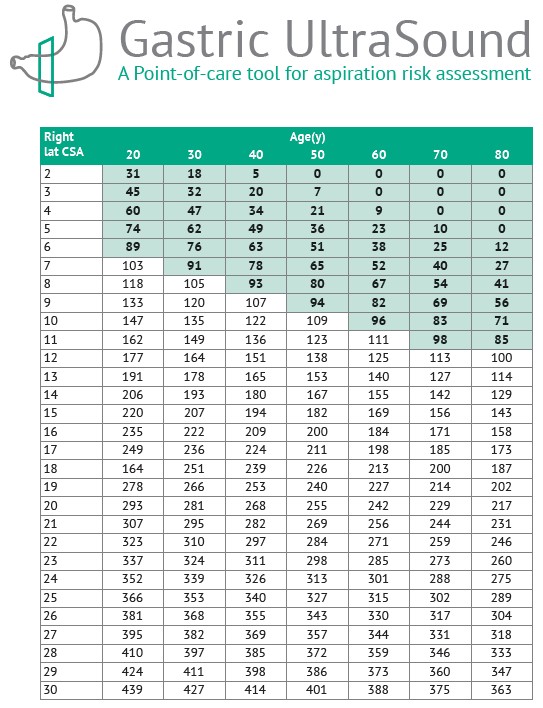
Figure 4. Gastric volume as a function of the antral cross-sectional area measured in the right lateral decubitus position and patient age
Used with permission from gastricultrasound.org.
By combining a qualitative and quantitative evaluation (when indicated), the I-AIM framework for gastric POCUS has high diagnostic accuracy for a full stomach (Figure 5).3 In a blinded study on healthy human subjects with a simulated pretest probability of a full stomach of 50%, a positive gastric POCUS test (solid content or > 1.5 mL/kg of clear fluid) increased the probability of a true full stomach to about 98%, and a negative test (grade 0 antrum or < 1.5 mL/kg) decreased the probability to less than 0.01%.3
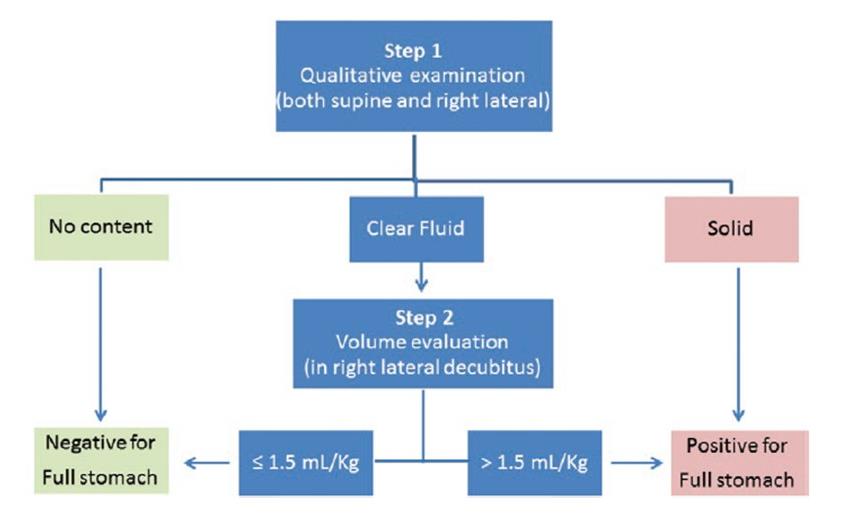
Figure 5. Schematic representation of the interpretation algorithm from gastric PoCUS findings
Used with permission from the Dr. Perlas Fontana Medicine Professional Corporation.
Medical Decision-Making
Gastric POCUS may be used to identify or rule out a full stomach when prandial status is unclear and thus guide safe anesthetic management.24,27 If the test is negative for a full stomach (grade 0 antrum or < 1.5 mL/kg of clear fluid), the surgical procedure may proceed as planned with no particular aspiration precautions. If, however, the test is positive for a full stomach (solid or thick fluid content or > 1.5 mL/kg of clear fluid), patient management may be individualized depending on the elective, urgent, or emergent nature of the surgical procedure. Postponing surgery is the most prudent decision in the setting of a full stomach if the surgery is elective or semiurgent but of low acuity (eg, closed fracture fixation).24,27 However, proceeding with surgery with full aspiration precautions may be warranted if the surgical procedure is urgent or emergent (eg, open fracture fixation, intracranial bleed, any situation with imminent risk to limb or life).28 Full aspiration precautions may include:
- Considering alternatives to general anesthesia
- Considering insertion of a nasogastric tube and suctioning preinduction, particularly if general anesthesia is required and gastric content is fluid in nature
- Avoiding an unprotected airway in the setting of deep sedation
- Securing the airway with endotracheal intubation and rapid sequence induction if general anesthesia is required
This summary described how we use gastric POCUS in the clinical setting to identify a full stomach when prandial status is equivocal, following an I-AIM framework to guide safe anesthetic management and prevent pulmonary aspiration of gastric contents.

Anahi Perlas, MD, FRCPC, is a staff anesthesiologist at Toronto Western Hospital and a professor in the department of Anesthesiology and Pain Medicine at the University of Toronto In Toronto, Canada.

Richelle Kruisselbrink, MD, FRCPC, is a staff anesthesiologist at Grand River Hospital and St. Mary's General Hospital in Kitchener and an assistant clinical professor at McMaster University in Hamilton, Canada.
References
- Perlas A, Mitsakakis N, Liu L, et al. Validation of a mathematical model for ultrasound assessment of gastric volume by gastroscopic examination. Anesth Analg 2013;116(2):357–63. https://doi.org/10.1213/ANE.0b013e318274fc19
- Kruisselbrink R, Arzola C, Endersby R, et al. Intra- and interrater reliability of ultrasound assessment of gastric volume. Anesthesiology 2014;121(1):46–51. https://doi.org/10.1097/aln.0000000000000193
- Kruisselbrink R, Gharapetian A, Chaparro LE, et al. Diagnostic accuracy of point-of-care gastric ultrasound. Anesth Analg 2019;128(1):89–95. https://doi.org/10.1213/ane.0000000000003372
- Perlas A, Chan V, Lupu M, et al. Ultrasound assessment of gastric content and volume. Anesthesiology 2009;111(1):82–9. https://doi.org/10.1093/bja/aeu151
- Perlas A, Davis L, Khan M, et al. Gastric sonography in the fasted surgical patient: a prospective descriptive study. Anesth Analg 2011;113(1):93–7. https://doi.org/10.1213/ane.0b013e31821b98c0
- Spencer AO, Walker AM, Yeung AK, et al. Ultrasound assessment of gastric volume in the fasted pediatric patient undergoing upper gastrointestinal endoscopy: development of a predictive model using endoscopically suctioned volumes. Paediatr Anaesth 2015;25(3):301–8. https://doi.org/10.1111/pan.12581
- Gagey AC, de Queiroz Siqueira M, Desgranges FP, et al. Ultrasound assessment of the gastric contents for the guidance of the anaesthetic strategy in infants with hypertrophic pyloric stenosis: a prospective cohort study. Br J Anaesth 2016;116(5):649–54. https://doi.org/10.1093/bja/aew070
- Schmitz A, Schmidt AR, Buehler PK, et al. Gastric ultrasound as a preoperative bedside test for residual gastric contents volume in children. Paediat Anaesth 2016;26(12):1157–64. https://doi.org/10.1111/pan.12993
- Arzola C, Cubillos J, Perlas A, et al. Inter-rater reliability and agreement of qualitative ultrasound assessment of gastric content in the third trimester of pregnancy. Br J Anaesth 2014;113(6):1018–23. https://doi.org/10.1093/bja/aeu257
- Arzola C, Perlas A, Siddiqui NT, et al. Bedside gastric ultrasonography in term pregnant women before elective cesarean delivery: a prospective cohort study. Anesth Analg 2015;121(3):752–8. https://doi.org/10.1213/ane.0000000000000818
- Rouget C, Chassard D, Bonnard C, et al. Changes in qualitative and quantitative ultrasound assessment of the gastric antrum before and after elective caesarean section in term pregnant women: a prospective cohort study. Anaesthesia 2016;71(11):1284–90. https://doi.org/10.1111/anae.13605
- Arzola C, Perlas A, Siddiqui NT, et al. Gastric ultrasound in the third trimester of pregnancy: a randomized controlled trial to develop a predictive model of volume assessment. Anaesthesia 2018;73(3):295–303. https://doi.org/10.1111/anae.14131
- Van de Putte P, Perlas A. Gastric sonography in the severely obese surgical patient: a feasibility study. Anesth Analg 2014;119(5):1105–10. https://doi.org/10.1213/ane.0000000000000373
- Kruisselbrink R, Arzola C, Jackson T, et al. Ultrasound assessment of gastric volume in severely obese individuals: a validation study. Br J Anaesth 2017;118(1):77–82. https://doi.org/10.1093/bja/aew400
- Bouvet L, Desgranges FP, Aubergy C, et al. Prevalence and factors predictive of full stomach in elective and emergency surgical patients: a prospective cohort study. Br J Anaesth 2017; 118(3):372–9. https://doi.org/10.1093/bja/aew462
- Bahner DP, Hughes D, Royall NA. I-AIM: a novel model for teaching and performing focused sonography. J Ultrasound Med 2012;31:295–300. https://doi.org/10.7863/jum.2012.31.2.295
- Perlas A, Van de Putte P, Van Houwe P, et al. I-AIM framework for point-of-care gastric ultrasound. Br J Anaesth 2016;116(1):7–11. https://doi.org/10.1093/bja/aev113
- Perlas A, Arzola C, Van de Putte P. Point-of-care gastric ultrasound and aspiration risk assessment: a narrative review. Can J Anaesth 2018;65(4):437–48. https://doi.org/10.1007/s12630-017-1031-9
- Haskins SC, Kruisselbrink R, Boublik J, et al. Gastric ultrasound for the regional anesthesiologist and pain specialist. Reg Anesth Pain Med 2018;43(7):689–98. https://doi.org/10.1097/aap.0000000000000846
- Lienhart A, Auroy Y, Pequignot F, et al. Survey of anesthesia-related mortality in France. Anesthesiology 2006;105:1087–97. https://doi.org/10.1097/00000542-200612000-00008
- Warner MA, Warner ME, Weber JG. Clinical significance of pulmonary aspiration during the perioperative period. Anesthesiology 1993;78:56–62. https://doi.org/10.1097/00000542-199301000-00010
- Cook TM, Woodall N, Frerk C, et al. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: anaesthesia. Br J Anaesth 2011;106:617–31. https://doi.org/10.1093/bja/aer058
- Sakai T, Planinsic RM, Quinlan JJ, et al. The incidence and outcomes of perioperative pulmonary aspiration in a university hospital: a four-year retrospective analysis. Anesth Analg 2006;103:941–7. https://doi.org/10.1213/01.ane.0000237296.57941.e7
- Alakkad H, Kruisselbrink R, Chin KJ, et al. Point-of-care ultrasound defines gastric content and changes the anesthetic management of elective surgical patients who have not followed fasting instructions: a prospective case series. Can J Anaesth 2015; 62(11):1188–95. https://doi.org/10.1007/s12630-015-0449-1
- Van de Putte P, Perlas A. Ultrasound assessment of gastric content and volume. Br J Anaesth 2014;113(1):12–22. https://doi.org/10.1093/bja/aeu151
- Cubillos J, Tse C, Chan VW, et al. Bedside ultrasound assessment of gastric content: an observational study. Can J Anaesth 2012;59(4):416–23. https://doi.org/10.1007/s12630-011-9661-9
- Van de Putte P, Vernieuwe L, Jerjir A, et al. When fasted is not empty: a retrospective cohort study of gastric content in fasted surgical patients. Br J Anaesth 2017;118(3): 363–71. https://doi.org/10.1093/bja/aew435
- Gagey AC, de Queiroz Siqueira M, Monard C, et al. The effect of pre-operative gastric ultrasound examination on the choice of general anaesthetic induction technique for non-elective paediatric surgery. A prospective cohort study. Anaesthesia 2018; 73(3):304–12. https://doi.org/10.1111/anae.14179
Leave a commentOrder by
Newest on top Oldest on top