Considerations for Starting an Outpatient Adductor Canal Catheter Program
Cite as: Gleicher Y, Kruisselbrink R. Considerations for starting an outpatient adductor canal catheter program. ASRA Pain Medicine News 2022;47. https://doi.org/10.52211/asra050122.017
Introduction
Total knee arthroplasty (TKA) is one of the most common surgical procedures in North America with approximately one million TKAs performed in 2020 in the United States.1,2 TKA has evolved into a short-stay inpatient procedure and, in recent years, many arthroplasty centers have started developing ambulatory TKA (ie, same-day discharge) pathways as well.3,4 Although pain is a major barrier for patient recovery and rehabilitation,4,5 nerve block techniques have gradually become a key component of post TKA analgesia and have decreased the opioid requirement of patients.6 With the adductor canal block (ACB) offering effective analgesia without quadricep weakness,7 it has become the mainstay of post TKA analgesia, with some arthroplasty centers beginning to offer continuous adductor canal block (CACB) analgesia to patients in an outpatient (ie, ambulatory) setting.8,9 Although the concept of outpatient continuous nerve block analgesia is not new,10-12 CACB in an outpatient setting provides a new set of considerations and challenges. This discussion will review these considerations.
Who Should Receive An Outpatient CACB?
Any patient undergoing TKA will likely benefit from CACB in the outpatient setting, but patients at risk for opioid-associated complications or tolerance may have even greater benefit. Patients, or a reliable live-in family member, need to understand instructions for self-monitoring of side effects and complications, respond to post-discharge phone calls, and follow directions for catheter removal. Outpatient CACBs benefit not only same-day discharge TKAs but also patients discharged postoperative day (POD) 1 or 2.9 At our centers, most patients going home on POD 1 or 2 are discharged with a CACB.
Equipment and Catheter Insertion
There are a variety of nerve block catheters that can be used for CACB. Catheter-through-needle (CTN) is a common approach and facilitates over-threading the catheter past the needle tip to prevent catheter dislodgement from the canal. Alternatively, some evidence suggests that a catheter-over-needle (CON) approach reduces the rate of catheter leakage and dislodgement at the skin.13 Our experience, by using sonographic assessment of catheters on PODs 0-2, is that catheters can dislodge out of the canal even with CON. We have found that the ability to over-thread the catheter tip inside the canal is important, achieved using an oblique insertion approach or by over-threading the catheter into the interfascial plane between the sartorius muscle and femoral artery (ISAFE approach).7 When over-threading is not possible, we found that feeding additional catheter into the sartorius muscle as the needle is withdrawn reduces canal dislodgement by creating “slack” between the catheter fixation points at the skin and the vasto-adductor membrane. Displacement (either out of the canal or intravascularly) by the intraoperative tourniquet or surgical knee manipulation is possible, and, in the outpatient setting, can have serious consequences. Therefore, to prevent intraoperative catheter dislodgement, providers can consider placing the catheter higher up in the proximal adductor canal if done preoperatively, or in the recovery room in the postoperative period. Additionally, if the catheter is placed preoperatively, we recommend that the position be verified postoperatively so that any migrated catheters can be re-sited prior to patient discharge.
There are many commercial infusion pump options for outpatient nerve catheters. Elastomeric infusion pumps deliver the local anesthetic at a fixed rate determined by a flow restrictor and the positive pressure of the elastomeric membrane (Figure 1). These single-use pumps provide a logistically simple option as they can usually be purchased pre-filled with a preferred local anesthetic and discarded once the catheter is removed. Costs typically range from $50 to $150 depending on the size of the pump and whether they come pre-filled. Depending on the manufacturer and brand, a wearable disposable sleeve for the pump may be available. Electronic pumps are an alternative option but require a larger capital investment, ongoing maintenance, and returning the pump to the surgical center after catheter removal. The advantage is the allowance of a customizable infusion rate by the care provider.

Figure 1. Adductor Canal Catheter. Example of adductor canal catheter secured to skin and attached to elastomeric pump. The pump is later inserted into a wearable sleeve that will allow the patient to ambulate while connected to the infusion pump.
When deciding on concentration and infusion rate of the local anesthetic, providers should consider potential complications. Higher doses may increase the risk of quadricep weakness and local anesthetic systemic toxicity (LAST). Previously investigated CACB infusion rates range from 5 ml-8 ml per hour and have been deemed to be safe.7 The duration of infusion depends on the reservoir size of the infusion pump. Commercially available elastomeric pump reservoirs typically range from 250 ml-600 ml and, depending on the flow rate, can facilitate 48-96 hours of CACB infusion. We recommend a minimum of 48 hours of postoperative CACB infusion, but care providers may consider longer infusions to minimize the occurrence of rebound pain upon CACB discontinuation.14 Since catheters stay in-situ for at least 2 days, all catheters should be secured with liquid adhesives and sterile adhesive strips to prevent dislodgement and leakage.
Complementary Multimodal Analgesia
The CACB will not cover all sources of pain post TKA, and patients may describe pain behind the knee as well as thigh pain if a tourniquet was used. Catheter dislodgement can occur as time progresses and patients mobilize. Therefore, all TKA patients should receive oral multimodal analgesia in addition to the CACB. Typically, this includes acetaminophen and an anti-inflammatory such as a cyclooxygenase 2 (COX2) inhibitor. A prescription for breakthrough opioids should always be provided. Despite the potential need for breakthrough opioids, our institution has found that in the outpatient setting, CACB significantly reduces opioid requirements, with more than 50% of same-day discharge patients not requiring opioids during the first 72 hours postoperatively.8
Local Anesthetic Systemic Toxicity (LAST)
LAST has been reported in association with ACBs but is most likely to occur due to intravascular injection during the initial bolus rather than the subsequent infusion.15 However, given the outpatient nature of this intervention, LAST prevention is of utmost importance. We recommend injecting saline or local anesthetic mixed with epinephrine 2.5 mcg/ml during catheter placement to detect intravascular uptake of injectate fluid, as well as choosing a catheter with a soft tip. The ISAFE approach to CACB catheter placement could reduce risk of femoral vein puncture and intravascular catheter migration by placing the catheter tip away from the femoral vein.8 In our combined experience of more than 600 outpatient catheters, we have not seen any LAST.
Quadriceps Weakness
As with LAST, quadriceps weakness is most likely to occur from the initial bolus of local anesthetic. A physiotherapy assessment prior to discharge is critical to minimize falls and ensure mobility discharge criteria are met. It also establishes a “baseline” mobility assessment.
Patient Monitoring and Follow-up
Patient education (Figure 2) and follow-up are critical components of a successful outpatient peripheral nerve catheter program. Virtual care follow-up can be provided by daily post-discharge phone calls. The assessment should include questions regarding the quality of analgesia, side effects including quadriceps weakness and LAST, and the integrity of the catheter dressing and connections. Patient education should also reinforce oral multimodal analgesia, use of cryotherapy, catheter care, and, when appropriate, the steps of catheter removal.
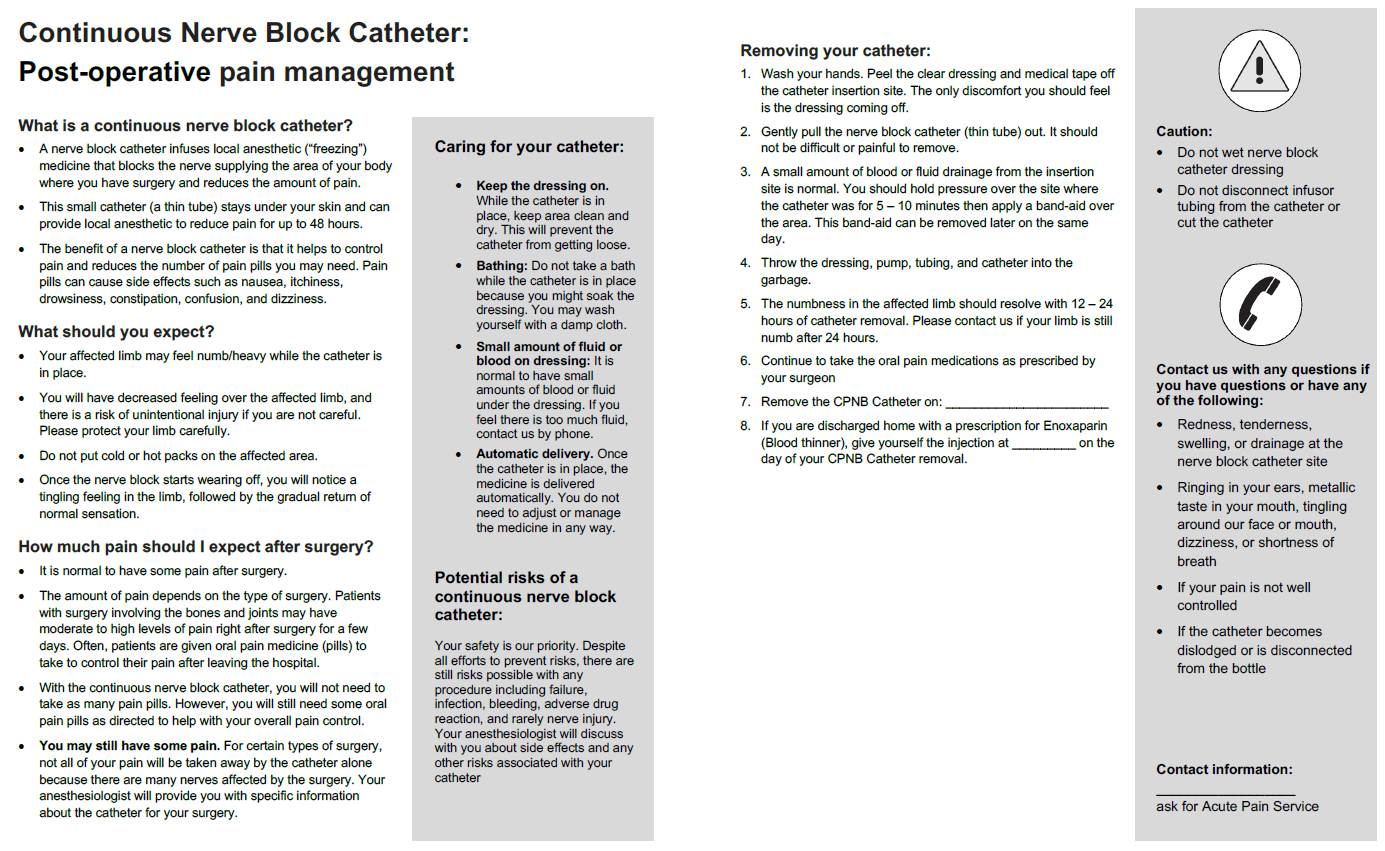
Figure 2. Patient Education Sheet
(courtesy of the Sinai Health Acute Pain Service). Download PDF
Patients should be given an emergency contact number along with instructions for appropriate use. In our experience, the emergency contact is rarely used as the virtual follow-ups are very effective. Patients should receive verbal and written instructions in case they experience symptoms of LAST, including discontinuing the infusion and calling for help. We recommend calling the emergency contact number for early signs, such as isolated tinnitus, and the emergency medical response services for more severe symptoms to facilitate timely assessment and treatment.
Catheter Removal
Patients are provided verbal and written instructions for catheter removal. More recently, we began explaining catheter removal by showing them a video of this process. Since TKA patients routinely receive postoperative deep vein thrombosis (DVT) prophylaxis, we advise patients to apply pressure at the insertion site for 5 minutes after catheter removal and to contact us should signs of a hematoma occur. The risk of a clinically significant hematoma after CACB nerve block catheter removal is very low but may vary depending on anticoagulation regimen.16 Given that the site of catheter insertion is compressible and relatively superficial, we believe and have found that catheter removal at home is safe within the context of DVT prophylaxis and aligns with the ASRA Pain Medicine anticoagulation guidelines.17
Summary
At our respective institutions, we have found that CACBs for TKA patients are safe and utterly transform patients’ TKA experience. We hope that our experience encourages other institutions to consider similar programs.

Yehoshua (Josh) Gleicher, MD, MSc, FRCPC, is the co-lead of Regional Anesthesia at Sinai Health and assistant professor and director of Quality and Safety in the department of Anesthesiology and Pain Medicine at the University of Toronto in Toronto, Canada.

Richelle Kruisselbrink, MD, FRCPC, is the Regional Anesthesia Lead at Grand River Hospital and assistant professor at McMaster University in Hamilton, Canada.
References
- Singh JA, Yu S, Chen L, Cleveland, JD. Rates of total joint replacement in the United States: future projections to 2020-2040 using the national inpatient sample. J Rheumatol 2019;46:1134–40. https://doi.org/10.3899/jrheum.170990
- Price AJ, Alvand A, Troelsen A, et al. Knee replacement. Lancet 2018;392:1672–82. https://doi.org/10.1016/S0140-6736(18)32344-4
- Bodrogi A, Dervin GF, Beaulé PE. Management of patients undergoing same-day discharge primary total hip and knee arthroplasty. CAMJ 2020;192(2):E34-9. https://doi.org/10.1503/cmaj.190182
- Cullom C, Weed JT. Anesthetic and analgesic management for outpatient knee arthroplasty. Curr Pain Headache Rep 2017;21:23. https://doi.org/10.1007/s11916-017-0623-y
- Hoffmann JD, Kusnezov NA, Dunn JC, et al. The shift to same-day outpatient joint arthroplasty: a systematic review. J Arthroplasty 2018;33:1265–74. https://doi.org/10.1016/j.arth.2017.11.027
- Summers S, Mohile N, McNamara C, et al. Analgesia in total knee arthroplasty: current pain control modalities and outcomes. J Bone and Joint Surg 2020;102:719-27. https://doi.org./10.2106/JBJS.19.01035
- Yu R, Wang H, Zhuo Y, et al. Continuous adductor canal block provides better performance after total knee arthroplasty compared with the single-shot adductor canal block? an updated meta-analysis of randomized controlled trials. Johns Hopkins Med J Supp 2020;99:e22762. https://doi.org/10.1097/MD.0000000000022762
- dos Santos Fernandes H, Siddiqui N, Peacock S, et al. Inter-fascial space between SArtorius muscle and FEmoral artery (ISAFE): a suggested approach for Adductor Canal catheter placement. J Clin Anesth 2022;76:110571. https://doi.org/10.1016/j.jclinane.2021.110571
- Hanson NA, Lee PH, Yuan SC, et al. Continuous ambulatory adductor canal catheters for patients undergoing knee arthroplasty surgery. J Clin Anesth 2016;35:190-4. https://doi.org/10.1016/j.jclinane.2016.07.022
- Fredrickson MJ, Ball CM, Dalgleish AJ. Successful continuous interscalene analgesia for ambulatory shoulder surgery in a private practice setting. Reg Anesth Pain Med 2008;33(2):122-8. https://doi.org/10.1016/j.rapm.2007.09.007
- Ilfeld, B.M., Vandenborne, K., Duncan, P.W., et al. Ambulatory continuous interscalene nerve blocks decrease the time to discharge readiness after total shoulder arthroplasty: a randomized, triple-masked, placebo-controlled study. Anesthesiology 2006;105(5):999-1007. https://doi.org/10.1097/00000542-200611000-00022
- Ma HH, Chou TF, Tsai SW, et al. The efficacy and safety of continuous versus single-injection popliteal sciatic nerve block in outpatient foot and ankle surgery: a systematic review and meta-analysis. BMC Musculoskelet Disord 2019;20:441. https://doi.org/10.1186/s12891-019-2822-7
- Edwards RM, Currigan DA, Bradbeer S, et al. Does a catheter over needle system reduce infusate leak in continuous peripheral nerve blockade: a randomised controlled trial. Anaesth intensive care 2018;46(5):468-73. https://doi.org/10.1177/0310057X1804600507
- Williams BA, Bottegal MT, Kentor ML, et al. Rebound pain scores as a function of femoral nerve block duration after anterior cruciate ligament reconstruction: retrospective analysis of a prospective, randomized clinical trial. Reg Anesth Pain Med 2007;32(3):186-92. https://doi.org/10.1016/j.rapm.2006.10.011
- Gleicher Y, Peacock S. Local anesthetic systemic toxicity following adductor canal block. Reg Anesth Pain Med 2019;44:973-4. https://doi.org/10.1136/rapm-2019-100610
- Idestrup C, Sawhney M, Nix C, et al. The incidence of hematoma formation in patients with continuous femoral catheters following total knee arthroplasty while receiving rivaroxaban as thromboprophylaxis: an observational study. Reg Anesth Pain Med 2014;39(5):414-7. https://doi.org/10.1097/AAP.0000000000000127
- Horlocker TT, Vandermeuelen E, Kopp SL, et al. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Fourth Edition). Reg Anesth Pain Med 2018;43(3):263-309. https://doi.org/10.1097/AAP.0000000000000763
Leave a commentOrder by
Newest on top Oldest on top