Peripheral Nerve Blocks of the Distal Upper Extremity
Authors
Sayeh Hamzehzadeh, MD
Resident Physician
E. David Bravos MD
Assistant Professor
Department of Anesthesiology and Critical Care Medicine
Johns Hopkins Hospital
School of Medicine, Johns Hopkins University
Baltimore, MD
Introduction
This review is devoted to peripheral nerve blocks of the distal upper extremity, specifically, those of the median, radial and ulnar nerves. These blocks are fairly simple to perform even by a beginner to produce anesthesia or analgesia for surgery of the forearm, wrist and hand. They may be done when blockade of the entire brachial plexus is not necessary, or as a “rescue” block with an incomplete brachial plexus block. Traditionally, these blocks have been performed at the level of the elbow and wrist using surface landmarks with nerve stimulation or paresthesia techniques.[1-2] More recently, ultrasound has been used to block the nerves at several different points between the elbow and wrist.[3]
Indications
Radial, ulnar and median nerve blocks can be performed alone or combined to provide intraoperative anesthesia or post-operative analgesia for surgical procedures of the forearm, wrist and hand. Such surgical procedures include carpel tunnel release, wrist arthroscopy, finger fracture, lacerations and tendon repairs.
Median Nerve
Anatomy
The median nerve travels towards the cubital fossa medial to the brachial artery and anterior to the brachialis muscle. At the cubital fossa, the nerve lies behind the bicipital aponeurosis and the medial cubital vein, just in front of the insertion of the brachialis muscle.
The median nerve is responsible for motor innervation to the flexor and pronator muscles of the forearm as well as the first two lumbricals and thenar muscles. Sensory innervation is provided to the palmar aspect of the thumb and second, third and lateral half of the fourth digit.
Techniques
Anatomic Landmark / Paresthesia
Positioning for a median nerve block at the elbow is done with the patient supine and the arm abducted at 90 degrees at the shoulder. The needle insertion site is perpendicular to the skin, 2 cm above the antecubital crease, medial to the brachial artery and biceps tendon. A 22 or 25-gauge 3.8 cm needle is advanced until paresthesia is elicited. 3–5 mL of local anesthetic solution can be injected into this space.
The median nerve block can also be performed at the wrist by locating the nerve between the palmaris longus and flexor carpi radialis tendons. These tendons are more visible by having the patient make a fist and flex at the wrist. A 22 or 25-gauge, 3.8 cm needle is advanced perpendicular to the skin between the two tendons until paresthesia is observed. A volume of 3–5 mL of local anesthetic solution is injected. If paresthesia is not noted the needle is advanced until bone contact is made, as which time while slowly removing the needle 3–5 mL of local anesthetic solution is delivered (Figure 1).
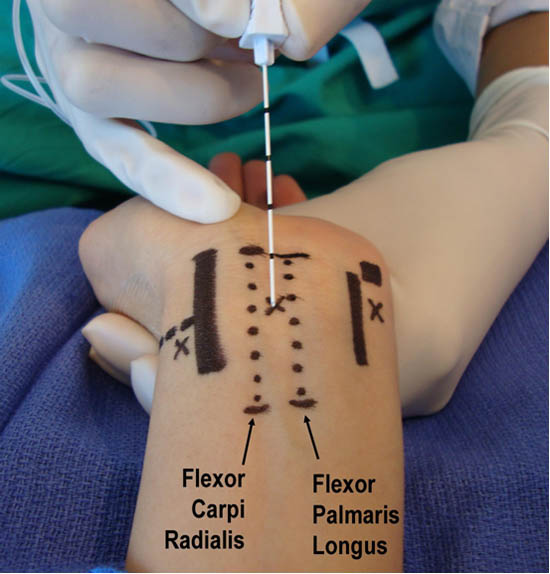 Figure 1. Median nerve blockade at the wrist
Figure 1. Median nerve blockade at the wrist
Nerve Stimulation
When using nerve stimulation the same anatomic landmarks for the median nerve are identified. The appropriate motor response would be wrist flexion or thumb opposition.
Ultrasound Guidance
Ultrasound-guided blockade of the median nerve can be performed at various points along its course between the elbow and wrist but it is best accomplished at the mid distal forearm.[3] In this location, it is easier to avoid the brachial artery as well as tendons, which can appear similar to nerves under ultrasound. In the mid distal forearm the nerve is visible between the flexor digitorum superficialis and the flexor digitorum profundus. Another ultrasound technique is to locate the ulnar nerve and artery under the flexor digitorum superficialis at the level of the mid forearm and then trace the muscle layer laterally until the median nerve is located. It is also possible to block both the median and ulnar nerve at this location (Figure 2).[1-3]
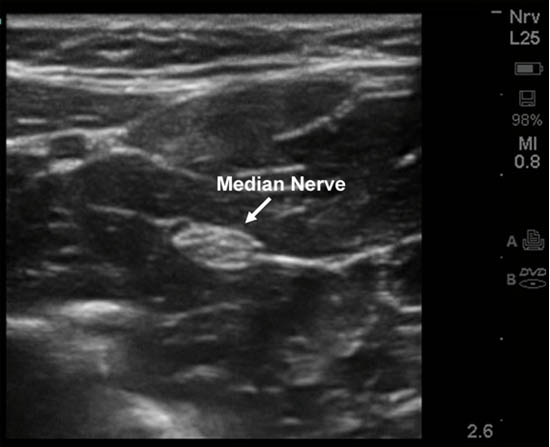
Figure 2. Ultrasound-guided median nerve blockade in the forearm
Radial Nerve
Anatomy
The radial nerve courses from the posterior aspect of the upper arm to a more lateral position near the elbow. At this level, it can be found between the brachialis and brachoradialis muscles. It then courses into the forearm dividing into a superficial sensory branch and a deeper motor branch. At the level of the wrist, the superficial radial nerve lies immediately below the styloid process of the radius in the anatomic snuff box superficial to the extensor pollicis longus tendon. The radial nerve can be located at various points along its course between the elbow and wrist using ultrasound.
In the forearm, the radial nerve provides motor innervation to the extensor muscles of the wrist and hand. Sensory innervation is provided to the posterior surface of the forearm and hand. The superficial branch of the radial nerve innervates the dorsum of the thumb, second, third and lateral aspect of the fourth finger.
Techniques
Anatomic Landmark/Paresthesia
To perform a radial nerve block at the level of the elbow, the patient should be positioned supine with the arm abducted. A 22 or 25-gauge 3.8 cm needle is advanced 2 cm lateral to the biceps tendon at the level of the epicondyles until paresthesia is elicited. At this location 5–7 mL of local anesthetic solution can be administered (Figure 3).
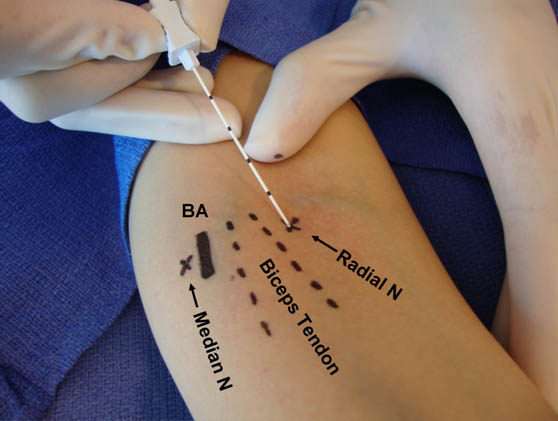 Figure 3. Radial nerve blockade at the elbow; BA = Brachial Artery
Figure 3. Radial nerve blockade at the elbow; BA = Brachial Artery
Radial nerve blocks performed at the wrist are done with the patient’s arm abducted 90 degrees and the hand in neutral position. At the level of the wrist, a field block of the radial nerve is performed in order to infiltrate its multiple peripheral branches. This is carried out with injection of 5–7 mL of local anesthetic around the anatomic snuff box superficial to the extensor pollicis longus tendon.
Nerve Stimulation
Using the same anatomical landmarks, nerve stimulation can be used to deposit local anesthetic around the radial nerve. At the level of the elbow, a positive response would include wrist extension and at the level of the wrist, extension of the fingers should be seen.
Ultrasound Guidance
The ideal location for finding the radial nerve without ultrasound guidance is at the elbow. With ultrasound guidance the nerve is visible deep to the brachioradialis muscle. The radial nerve may be difficult to follow distally from the elbow, and at best only the superficial branch can be visualized.[3] One injection at this site may block both the deep and superficial branches of the radial nerve (Figure 4).
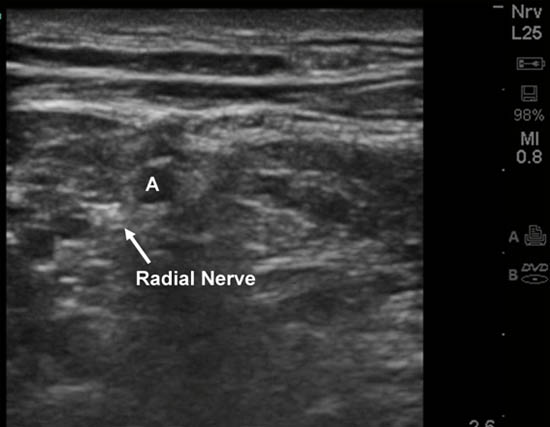
Figure 4. Ultrasound-guided radial nerve blockade in the forearm.
Ulnar Nerve
Anatomy
The ulnar nerve descends from the posteriormedial aspect of the humerus and at the level of the elbow can be located superficially at the bony canal between the medial epicondyle and the olecranon process in the ulnar groove. The nerve continues to descend into the forearm in the anterior compartment where it then enters the hand medial to the ulnar artery and lateral to the flexor carpi ulnaris tendon at the wrist level. The ulnar nerve can be located at various points along its course between the elbow and wrist using ultrasound.
The ulnar nerve provides motor innervation to the intrinsic muscles of the hand, as well as the flexor carpi ulnaris. Sensory innervation includes the medial half of the palm as well as the fifth and part of the fourth finger.
Techniques
Anatomic Landmark / Paresthesia
Ulnar nerve blockade can be performed at the elbow or wrist. When performed at the elbow, the patient should be supine with the forearm flexed at the elbow onto the upper arm. The ulnar groove can be easily palpated between the medical epicondyle and olecranon process. A 22 or 25 gauge 3.8 cm needle is inserted 1 cm proximal to the junction of the olecranon process and the medial epicondyle and directed distally. Paresthesia may or may not be elicited. The needle is withdrawn 1 mm and 3-5 mL of local anesthetic solution is injected. Large volume of local anesthetic should be avoided for this particular block secondary to high pressure that could develop in this fascial compartment causing neural injury (Figure 5).
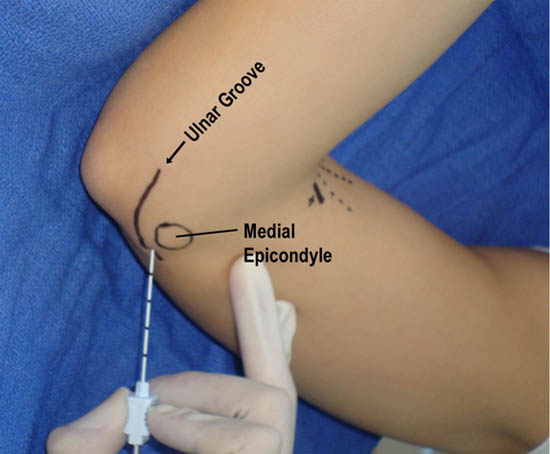 Figure 5. Ulnar nerve blockade at the elbow
Figure 5. Ulnar nerve blockade at the elbow
To perform an ulnar nerve block at the wrist, palpate the flexor carpi ulnaris tendon and the ulnar artery just proximal to the ulnar styloid process. Local anesthetic solution of 3–5 mL is injected. If it is difficult to elicit paresthesia, the local anesthetic solution can be injected in a fan-like fashion between the artery and tendon (Figure 6).
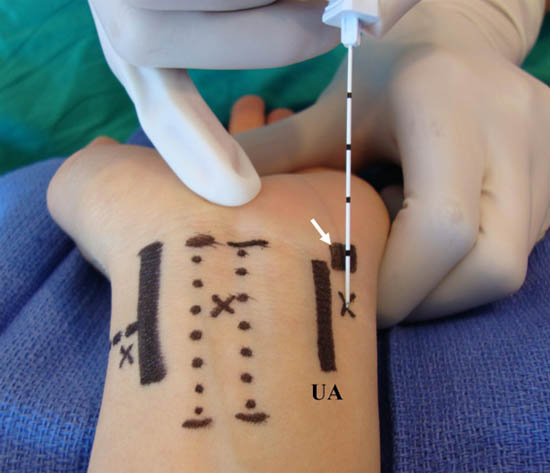 Figure 6. Ulnar nerve blockade at the wrist; UA = Ulnar Artery
Figure 6. Ulnar nerve blockade at the wrist; UA = Ulnar Artery
Nerve Stimulation
Using the same anatomical landmarks, nerve stimulation can be used to deposit local anesthetic around the ulnar nerve. Motor response observed for an ulnar nerve block at the elbow would include adduction of the hand or flexion of the fourth and fifth finger.
Ultrasound Guidance
Ultrasound guidance for ulnar nerve block is best performed at the mid forearm where it is more easily seen.[3] At this level, the nerve is medial to the ulnar artery and proximal to the origin of its dorsal branch, thus ensuring adequate blockade. A 5 mL solution of local anesthetic should be injected around the nerve to ensure a complete block (Figure 7).
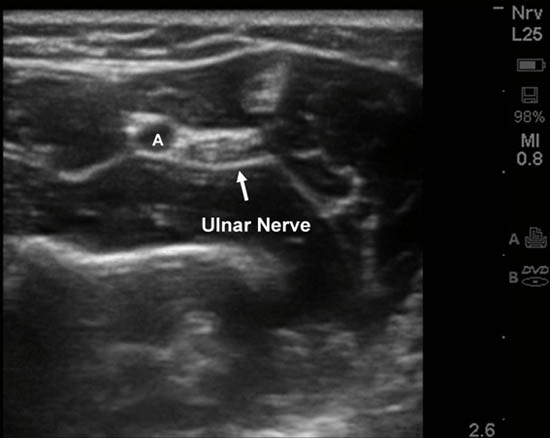 Figure 7. Ultrasound-guided ulnar nerve blockade in the forearm.
Figure 7. Ultrasound-guided ulnar nerve blockade in the forearm.
Local Anesthetic
Choice of local anesthetic solutions is mainly based on whether the block is being done for anesthesia or analgesia. Common characteristic considered are the onset and duration of local anesthetic to accomplish this.
Complications
General complications for these peripheral nerve blocks include infection, bleeding, nerve injury and local anesthetic toxicity.
To decrease the risk of infection, the clinician should always use an aseptic technique.[5] Bleeding and vascular injury can occur especially if a nerve is in close proximity to a vessel. The use of ultrasound may decrease this risk. The risk of local anesthetic toxicity is always a possibility with peripheral nerve blocks and may be slightly smaller given the smaller volumes of local anesthetic used for these blocks.
Nerve injury is always a risk of peripheral nerve blocks that can be from several different mechanisms. It is thought that these blocks may carry a potentially higher risk when performed at the elbow or wrist given the surrounding structures that may "compartmentalize" the nerve making it more vulnerable to a compression injury. Additionally, if these blocks are done as a "rescue" to an incomplete proximal brachial plexus block, it is possible that the patient is less capable of perceiving paresthesia or pain on injection of the local anesthetic solution.[1]
Summary
Peripheral nerve blocks of the distal upper extremity are a useful skill set to utilize when there is a need to supplement a brachial plexus block. Historically these blocks have been performed using surface landmarks, however now the efficacy and safety of these blocks can potentially be improved with the utilization of ultrasound guidance. It is important to be familiar the anatomic distribution of the peripheral nerves in order to best meet the anesthetic demands of the surgical procedure.
References
- Neal J. Cutaneous Blocks for the Upper extremity: Textbook of Regional Anesthesia and Acute Pain Management. McGraw Hill, 2007: 467-475.
- Brown DL: Distal Upper Extremity Blocks: Atlas of Regional Anesthesia 3rd edition, Saunders 2006: 71-79.
- McCartney C, Xu D, Constantinescu C, Sherif A, et al. Ultrasound examination of peripheral nerves in the forearm. Reg Anesth Pain Med 2007;32:343-439.
- Marhofer P: Upper extremity peripheral blocks. Techniques in Regional Anesthesia and Pain Management 2007;11:215-221.
- Hebl, JR. The importance and implications of aseptic techniques during regional anesthesia. Reg Anesth Pain Med 2006;31:311-323.
Leave a commentOrder by
Newest on top Oldest on top