Autonomic Modulation’s Emerging Role in Post-Acute Sequelae of SARS-CoV-2 Infection
Cite as: Ganesh A, Agarwal S, Qadri Y. Autonomic modulation's emerging role in post-acute sequelae of SARS-CoV-2 infection. ASRA Pain Medicine News 2022;47. https://doi.org/10.52211/asra110122.047
Post-acute sequelae of SARS-CoV-2 infection (PASC), commonly referred to as long COVID, encompasses a variety of symptoms that persist in a patient months after infection with the SARS-CoV-2 virus.1 Approximately 10%–20% of patients report multisystem long-term effects such as fatigue, cognitive impairment, headache, loss of smell or taste, depression, palpitations, diarrhea, or muscle or joint pain (see Figure 1). These symptoms are generally managed with a multidisciplinary approach involving medications, treatment of underlying or contributory disorders, physical and cognitive therapy, and in some centers, use of novel interventions such as sympathetic blocks or neuromodulation.3,4
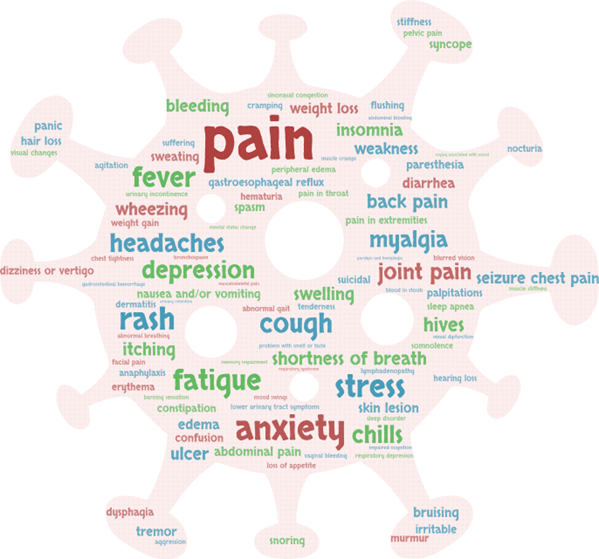
Figure 1. Word cloud illustration of the top 100 PASC symptoms, with each term’s relative size representing the frequency of patient reports2
What Is PASC?
The diagnostic criteria for PASC are still developing, but it is generally described as a constellation of symptoms that some patients experience approximately one to three months after SARS-CoV-2 infection secondary to either end-organ damage from the infection, hospitalization, or treatments. 1,5 Most definitions identify PASC as a diagnosis of exclusion, and some describe symptoms that may wax and wane. PASC’s mechanism is nebulous, with theories postulating persistent viral infection or hypercoagulability and immune dysregulation. The breadth of symptoms and proposed mechanisms present challenges for treatment, but an association between the nervous system and PASC may help clinicians and researchers identify new approaches.
One primary area where sympathetic blocks may have benefit are PASC’s olfactory symptoms.
The Nervous System’s Role in Acute SARS-CoV-2 Infections
Although some PASC effects can be postulated to be to direct viral infection of neurons, SARS-CoV-2 infection is known to robustly affect neuronal tissue via cytokines released by immune cells such as macrophages or T cells.6 This is most clearly demonstrated mechanistically in symptoms such as smell or taste disturbances, where murine models of olfactory receptor expression in neurons show relatively low correlation between neuron infection and magnitude of receptor expression change.7
The autonomic and somatic nervous systems are not commonly discussed as contributing factors to infection pathogenesis. However, a growing body of literature identifies communication between neurons and immune system cells and suggests a benefit to manipulation of neuronal systems in infectious states. For example, preclinical murine models show that chemical ablation of transient receptor potential vanilloid 1–positive neurons in lung tissue protects against mortality and morbidity secondary to cytokine storm triggered by severe bacterial pneumonias. Clinically, a simple procedure such as a stellate ganglion block will alter immune cell subsets and activity within 30 minutes.8 Similarly, vagal nerve stimulation quiets the inflammatory reflex and is used as an electrical anti-inflammatory agent in various states.9,10
The possible application in SARS-CoV-2 led to new research and the formation of the International Consortium on Neuromodulation for COVID-19.3 Multiple clinical trials are studying therapies attempting to manipulate the autonomic nervous system in the acute setting, with early findings that noninvasive vagal stimulation may reduce markers of inflammation but not yet offer clear mortality or morbidity benefit.11–13
The Autonomic Nervous System’s Role in PASC
The autonomic nervous system may be the key to reducing PASC symptoms and possibly providing an overarching treatment. Blocks targeting the various autonomic ganglia have been used to treat sympathetically mediated pain and a plethora of other pathologies, including cerebral vasospasm, cardiac arrhythmias, vasospastic Raynaud’s disease, postural orthostatic tachycardia syndrome, post-traumatic stress disorder (PTSD), or hyperhidrosis.14–16
One primary area where sympathetic blocks may have benefit are PASC’s olfactory symptoms. Prior to the pandemic, a 2003 study showed remarkable efficacy with 70% of patients improving after persistent post-upper respiratory infection–related olfactory disorder recalcitrant to conventional therapies.17 The evidence for use of stellate ganglion blocks in those and other states of altered autonomic function (eg, complex regional pain syndrome, hot flashes, PTSD, insomnia) led Liu and Duricka to offer two patients with PASC a set of bilateral stellate ganglion blocks staggered over 24–48 hours.4 The patients showed marked subjective improvement in multiple domains of PASC symptoms that were maintained over a two-month follow-up period. Although these anecdotal data appear positive,4,18 randomized controlled trials or larger case series have yet to be published.
However, multiple providers are offering the procedures in clinics for patients with PASC symptoms. The overarching hypothesis is that sympathetic blocks trigger changes in the immune system, overall stress response, and possibly increased blood flow to target areas such as the sinuses or brain. Human studies have shown alterations in those variables with local anesthetic applied to the stellate ganglion, but the effect recedes within hours to days. Early reports of use in PASC do not seem to show abatement of the stellate ganglion block’s effects, and thus it is tempting to consider that PASC may be cured by resetting the autonomic system. The benefits for stellate ganglion blocks with local anesthetic for other states is limited, with data for hot flashes, PTSD, or pain suggesting a duration of days to weeks and rarely months. For some clinicians, this has led to surgical resection thermal ablation of the stellate ganglion if symptoms return or off-label use of botulinum toxin to obtain months rather than days to weeks of sympathetic blockade.19,20
Future Work
Thus far, a nervous system approach to PASC treatment has focused on a set of bilateral stellate ganglion blocks separated by a minimal amount of time for safety because of concern for bilateral recurrent laryngeal nerve blockade. As interdisciplinary teams develop and conduct more research, providers will likely assess the role of other sympathetic or parasympathetic blocks such as the sphenopalatine ganglion blocks for patients with primarily cranial symptoms, splanchnic nerve blocks for patients with primarily abdominal symptoms, hypogastric/ganglion of impar blocks for patients with pelvic symptomatology, or even trigger-point blocks to interrupt sympathetically mediated somatovisceral reflex arcs.18 Electrical neuromodulation of the vagus nerve or direct brain stimulation may also have a role.3
Although those questions and study avenues are provocative, the most urgent need is for a randomized clinical trial of sympathetic blocks for PASC. Stellate ganglion blocks for PTSD showed great benefit in large case series but have had mixed results in structured randomized controlled trials.16 One factor is the inherent challenges of studying a complex psychiatric state such as PTSD, and PASC is likely to have challenges as well. For example, although a stellate ganglion block produces readily noticeable physiologic effects such as Horner syndrome, a placebo-controlled trial may never be feasible. Subjective markers based on patient perception or even structured questionnaires can also lead to significant variability in results. An optimal approach is to measure trends in blood or cerebrospinal fluid biomarkers for PASC, but those are still being defined. The SARS-CoV-2 spike protein is currently a front-runner.21
Conclusions
Interactions between the immune and nervous system appear to drive the pathophysiology of acute and post-acute SARS-CoV-2 infection states. Modulating the nervous system may alleviate some of that pathophysiology, but more structured and rigorous research is needed for both acute and PASC.

Arun Ganesh, MD, is an assistant professor in the department of anesthesiology general, vascular, and transplant anesthesiology division at Duke University in Durham, NC.

Sunil Agarwal, MD, is a pain medicine fellow in the department of anesthesiology division of pain medicine at Emory University in Atlanta, GA.

Yawar J. Qadri, MD, PhD, is the director of interventional pain therapies and an assistant professor in the department of anesthesiology division of pain management at Emory University in Atlanta, GA.
References
- Castanares-Zapatero D, Chalon P, Kohn L, et al. Pathophysiology and mechanism of long COVID: a comprehensive review. Ann Med. 2022;54:1473–1487. https://doi.org/10.1080/07853890.2022.2076901
- Wang L, Foer D, MacPhaul E, Lo YC, Bates DW, Zhou L. PASCLex: A comprehensive post-acute sequelae of COVID-19 (PASC) symptom lexicon derived from electronic health record clinical notes. J Biomed Inform. 2022;125:103951. https://doi.org/10.1016/j.jbi.2021.103951
- Czura CJ, Bikson M, Charvet L, et al. Neuromodulation strategies to reduce inflammation and improve lung complications in COVID-19 patients. Front Neurol. 2022;13:897124. https://doi.org/10.3389/fneur.2022.897124
- Liu LD, Duricka DL. Stellate ganglion block reduces symptoms of long COVID: a case series. J Neuroimmunol. 2022;362:577784. https://doi.org/10.1016/j.jneuroim.2021.577784
- Chippa V, Aleem A, Anjum F. Post acute coronavirus (COVID-19) syndrome. In: Statpearls. Treasure Island (FL), 2022. https://www.ncbi.nlm.nih.gov/books/NBK570608
- De Virgiliis F, Di Giovanni S. Lung innervation in the eye of a cytokine storm: neuroimmune interactions and COVID-19. Nat Rev Neurol. 2020;16:645–652. https://doi.org/10.1038/s41582-020-0402-y
- Zazhytska M, Kodra A, Hoagland DA, et al. Non-cell-autonomous disruption of nuclear architecture as a potential cause of COVID-19-induced anosmia. Cell. 2022;185:1052–1064.e12. https://doi.org/10.1016/j.cell.2022.01.024
- Yokoyama M, Nakatsuka H, Itano Y, Hirakawa M. Stellate ganglion block modifies the distribution of lymphocyte subsets and natural-killer cell activity. Anesthesiology. 2000;92:109–15. https://doi.org/10.1097/00000542-200001000-00021
- Kwan H, Garzoni L, Liu HL, et al. Vagus nerve stimulation for treatment of inflammation: systematic review of animal models and clinical studies. Bioelectron Med. 2016;3:1–6. http://www.ncbi.nlm.nih.gov/pmc/articles/pmc5756070
- Patel ABU, Weber V, Gourine AV, Ackland GL. The potential for autonomic neuromodulation to reduce perioperative complications and pain: a systematic review and meta-analysis. Br J Anaesth. 2022;128:135–149. https://doi.org/10.1016/j.bja.2021.08.037
- Kaniusas E, Szeles JC, Kampusch S, et al. Non-invasive auricular vagus nerve stimulation as a potential treatment for Covid19-originated acute respiratory distress syndrome. Front Physiol. 2020;11:890. https://doi.org/10.3389/fphys.2020.00890
- Rangon CM, Barruet R, Mazouni A, et al. Auricular neuromodulation for mass vagus nerve stimulation: insights from SOS COVID-19 a multicentric, randomized, controlled, double-blind French pilot study. Front Physiol. 2021;12:704599. https://doi.org/10.3389/fphys.2021.704599
- Tornero C, Pastor E, Garzando MDM, et al. Non-invasive vagus nerve stimulation for COVID-19: results from a randomized controlled trial (SAVIOR I). Front Neurol. 2022;13:820864. https://doi.org/10.3389/fneur.2022.820864
- Brown B, Naber JW, Kapural L. Long-term control of abdominal pain related to POTS: two case reports in pediatrics. Pain Manag. 2018;8:437–440. https://doi.org/10.2217/pmt-2018-0013
- Ho KWD, Przkora R, Kumar S. Sphenopalatine ganglion: block, radiofrequency ablation and neurostimulation—a systematic review. J Headache Pain. 2017;18:118. https://doi.org/10.1186/s10194-017-0826-y
- Kerzner J, Liu H, Demchenko I, et al. Stellate ganglion block for psychiatric disorders: a systematic review of the clinical research landscape. Chronic Stress. 2021;5:24705470211055176. https://doi.org/10.1177/24705470211055176
- Park HJ, Kim DY, Bae JH, Lee SS. The effect of stellate ganglion block on the treatment of sensorineural olfactory disorder following upper respiratory tract infection. Korean J Otorhinolaryngol-Head Neck Surg. 2013;56:84–89. http://doi.org/10.3342/kjorl-hns.2013.56.2.84
- Vinyes D, Munoz-Sellart M, Caballero TG. Local anesthetics as a therapeutic tool for post COVID-19 patients: a case report. Medicine (Baltimore). 2022;101:e29358. https://doi.org/10.1097/md.0000000000029358
- Lee ACH, Tung R, Ferguson MK. Thoracoscopic sympathectomy decreases disease burden in patients with medically refractory ventricular arrhythmias. Interact Cardiovasc Thorac Surg. 2022;34:783–790. https://doi.org/10.1093/icvts/ivab372
- Yoo Y, Lee CS, Kim J, Jo D, Moon JY. Botulinum toxin type A for lumbar sympathetic ganglion block in complex regional pain syndrome: a randomized trial. Anesthesiology. 2022;136:314–325. https://doi.org/10.1097/aln.0000000000004084
- Swank Z, Senussi Y, Alter G, Walt DR. Persistent circulating SARS-CoV-2 spike is associated with post-acute COVID-19 sequelae. Clin Infect Dis. 2022;ciac722. https://doi.org/10.1093/cid/ciac722
Leave a commentOrder by
Newest on top Oldest on top